Saturday, May 07, 2011
Greenlight Laser Photovaporization
Greenlight Laser Photovaporization. .The Greenlight Laser Photovaporization is referred to by several names-PVP, Greenlight HPS, Greenlight PV, Photo-Selective Vaporization of the Prostate, Laser Prostatectomy and Laser TURP. While the names of this enlarged prostate gland surgical treatment may vary, the procedure itself is the same. This treatment option uses a laser to downsize the enlarged prostate gland by targeting the obstructive portion of the enlarged prostate gland and vaporizing it. The PVP laser, with fiber optic delivery, emits a green light and seals blood vessels during the procedure to lessen bleeding. The Greenlight Laser Photovaporization is a minimally invasive procedure, usually performed as outpatient surgery and the patient has immediate results in terms of urinary flow restoration. The Greenlight Laser Photovaporization treatment option reportedly does not cause deep tissue damage to the patient, so recovery time rapid and side effects are minimal
Wednesday, July 25, 2007
Enlarged prostate (BPH) guide - MayoClinic.com
Who it works best for. TUMT works best for men with moderately enlarged glands and moderate symptoms. It doesn't work as well if your prostate enlargement has occurred mainly in the gland's middle lobe, which grows upward and presses into your bladder. In such cases, the microwave antenna may not produce enough energy to reach the obstructing part of your prostate. Because of potential complications, TUMT isn't recommended if you have a penile implant, an artificial urinary sphincter or certain health problems. It's also not recommended if you have had radiation treatments in the pelvic area or if you have had pelvic surgery. If you have a pacemaker or an implanted defibrillator, you will need to consult with your cardiologist and see whether the device can be deactivated for the procedure. Your doctor will perform cystoscopy before deciding to use TUMT to be sure that your internal anatomy is suitable for the procedure.
Outcome. TUMT is more effective than medications at improving urine flow, but is less effective than is traditional prostate surgery (TURP). However, TUMT does improve urinary flow in most men who undergo the procedure. TUMT decreases symptom index scores an average of nine to 11 points, compared with 14 to 20 points for surgery. Some doctors consider TUMT the best choice among the minimally invasive treatments currently available.
Several weeks may pass before you see a noticeable improvement in your urinary symptoms. That's because your body needs time to break down and absorb overgrown prostate tissue that's been destroyed by the microwave energy. The long-term effectiveness of the procedure is still unknown.
Side effects. Painful urination can persist for several weeks after TUMT — until your body completely absorbs the destroyed prostate tissue. Most men require a catheter for a few days after the procedure.
Other side effects:
- Temporary urinary urgency or frequency may occur depending on the microwave device used and how likely it is to produce these side effects.
- Urinary tract infection occurs in some men. It's more likely to occur the longer you require a catheter.
- Narrowing (stricture) of the urethra may develop and may require additional treatment.
- Decreased amount of semen ejaculated may occur. TUMT rarely causes erection problems or incontinence. Retrograde ejaculation — a condition in which semen flows backward into the bladder during ejaculation — occurs in about one in five men who have the procedure.
Enlarged prostate (BPH) guide - MayoClinic.com: "Need for re-treatment. The need for additional treatment after TUMT is more likely than it is after standard surgery, either because symptoms return or because they never adequately improve. Some men who undergo TUMT later require more treatment — usually surgery."
Natural History and Treatment Options for Benign Prostatic Hyperplasia
Natural History and Treatment Options for Benign Prostatic Hyperplasia: "Treatment Options For An Enlarged Prostate
Watchful waiting is excellent treatment option for a large percentage of men with LUTS. Watchful waiting is appropriate in a man who has lower urinary tract symptoms which do not significantly bother him or interfere with his lifestyle and who maintains good bladder function and good bladder emptying. Most men who undergo watchful waiting should be seen by their physician on an annual basis and have an assessment of their urinary symptoms, a digital rectal exam to check the prostate for signs of cancer and a prostate specific antigen (PSA) blood test to evaluate for prostate cancer which may not be palpable on rectal exam. If a man’s symptoms worsen, he would then be offered treatment options that are discussed below. A large percentage of men can be managed for years, or their entire lives, with watchful waiting and never require aggressive treatment for their prostatic enlargement."
Watchful waiting is excellent treatment option for a large percentage of men with LUTS. Watchful waiting is appropriate in a man who has lower urinary tract symptoms which do not significantly bother him or interfere with his lifestyle and who maintains good bladder function and good bladder emptying. Most men who undergo watchful waiting should be seen by their physician on an annual basis and have an assessment of their urinary symptoms, a digital rectal exam to check the prostate for signs of cancer and a prostate specific antigen (PSA) blood test to evaluate for prostate cancer which may not be palpable on rectal exam. If a man’s symptoms worsen, he would then be offered treatment options that are discussed below. A large percentage of men can be managed for years, or their entire lives, with watchful waiting and never require aggressive treatment for their prostatic enlargement."
| |
Natural History and Treatment Options for Benign Prostatic HyperplasiaMichael J. Naslund, M.D. |
Transurethral microwave thermotherapy for the treatment of BPH: still a challenger?
Transurethral microwave thermotherapy for the treatment of BPH: still a challenger?: "World J Urol. 2006 Jun 3; : 16752156
Transurethral microwave thermotherapy for the treatment of BPH: still a challenger?
[My paper] T Herrmann , A Gross , D Schultheiss , P Kaufmann , U Jonas , M Burchardt
Minimally invasive therapies for treatment of benign prostatic hyperplasia (BPH) compete with the gold standard transurethral resection of the prostate (TURP). Comparisons of efficacy and safety have broadened the knowledge of different treatment modalities. Concerns of quality of life such as unaltered sexual function as well as cost considerations drive the market to develop techniques of lower level invasiveness. Among the competitors the office based transurethral microwave thermotherapy (TUMT) provides the broadest scale of scientific data. Numerous manufacturers sell various modifications of this technology. According to different clinical studies TUMT proved to be an effective, safe, and durable therapy for the treatment of lower urinary tract symptoms (LUTS) secondary to BPH. However, TURP still holds the steadier long-term results and is more effective to reduce obstruction as well as other LUTS."
Transurethral microwave thermotherapy for the treatment of BPH: still a challenger?
[My paper] T Herrmann , A Gross , D Schultheiss , P Kaufmann , U Jonas , M Burchardt
Minimally invasive therapies for treatment of benign prostatic hyperplasia (BPH) compete with the gold standard transurethral resection of the prostate (TURP). Comparisons of efficacy and safety have broadened the knowledge of different treatment modalities. Concerns of quality of life such as unaltered sexual function as well as cost considerations drive the market to develop techniques of lower level invasiveness. Among the competitors the office based transurethral microwave thermotherapy (TUMT) provides the broadest scale of scientific data. Numerous manufacturers sell various modifications of this technology. According to different clinical studies TUMT proved to be an effective, safe, and durable therapy for the treatment of lower urinary tract symptoms (LUTS) secondary to BPH. However, TURP still holds the steadier long-term results and is more effective to reduce obstruction as well as other LUTS."
A Randomized Study Comparing High–Energy TUMT to TURP: Quality–of–Life Results
Vol. 38, No. 5, 2000
 Medline Abstract (ID 11096238)
Medline Abstract (ID 11096238)
A Randomized Study Comparing High-Energy TUMT to TURP: Quality-of-Life Results
E.A.E. Franciscaa, F.C.H. d'Anconaa, J.C.M. Hendriksb, L.A.L.M. Kiemeneya,b, F.M.J. Debruynea, J.J.M.C.H de la Rosettea
Departments of
aUrology and
bEpidemiology and Biostatics, University Hospital Nijmegen, The Netherlands
A Randomized Study Comparing High–Energy TUMT to TURP: Quality–of–Life Results: "Results: For almost all scales the standardized Cronbach's alpha was adequate. Between the various QoL scales there is a statistically significant correlation except for social well-being and sexual functions. There is also a significant correlation between the QoL scales and age, IPSS and Madsen. For the sexual functions there is only a correlation with age. A significant difference in improvement in favor of the TURP group was observed in general perception of urinary difficulties and activities of daily living. However, no difference between the groups was observed for the QoL scale measuring experienced improvement. The sexual function is not influenced by both treatment modalities. Both groups have a significant improvement in clinical outcome at all points of measurement. TURP has a better clinical outcome.
Conclusion: Both TUMT and TURP have a significant positive effect on various aspects of QoL. In particular, perception of urinary difficulties and activities of daily living are positively influenced by both treatments. TURP, however, has a greater impact than high-energy TUMT.
goto top of page Author Contacts
E.A.E. Francisca
Department of Urology, University Hospital Nijmegen
PO Box 9101, NL-6500 HB Nijmegen (The Netherlands)
Tel. +31 24 3613920, Fax +31 24 3541031
E-Mail e.francisca@uro.azn.nl"
A Randomized Study Comparing High-Energy TUMT to TURP: Quality-of-Life Results
E.A.E. Franciscaa, F.C.H. d'Anconaa, J.C.M. Hendriksb, L.A.L.M. Kiemeneya,b, F.M.J. Debruynea, J.J.M.C.H de la Rosettea
Departments of
aUrology and
bEpidemiology and Biostatics, University Hospital Nijmegen, The Netherlands
A Randomized Study Comparing High–Energy TUMT to TURP: Quality–of–Life Results: "Results: For almost all scales the standardized Cronbach's alpha was adequate. Between the various QoL scales there is a statistically significant correlation except for social well-being and sexual functions. There is also a significant correlation between the QoL scales and age, IPSS and Madsen. For the sexual functions there is only a correlation with age. A significant difference in improvement in favor of the TURP group was observed in general perception of urinary difficulties and activities of daily living. However, no difference between the groups was observed for the QoL scale measuring experienced improvement. The sexual function is not influenced by both treatment modalities. Both groups have a significant improvement in clinical outcome at all points of measurement. TURP has a better clinical outcome.
Conclusion: Both TUMT and TURP have a significant positive effect on various aspects of QoL. In particular, perception of urinary difficulties and activities of daily living are positively influenced by both treatments. TURP, however, has a greater impact than high-energy TUMT.
goto top of page Author Contacts
E.A.E. Francisca
Department of Urology, University Hospital Nijmegen
PO Box 9101, NL-6500 HB Nijmegen (The Netherlands)
Tel. +31 24 3613920, Fax +31 24 3541031
E-Mail e.francisca@uro.azn.nl"
Wednesday, December 27, 2006
FDA: Microwave Thermotherapy for Benign Prostatic Hyperplasia
From: "Alonge, Laura A."
Subject: RE: Microwave Thermotherapy for Benign Prostatic Hyperplasia
Date: Wed, 27 Dec 2006 16:01:25 -0500
In October 2000, the FDA issued a Public Health Notification alerting clinicians to the possibility of serious, unanticipated adverse events associated with microwave thermotherapy for treatment of BPH ( http://www.fda.gov/cdrh/safety/bph.html ). One of the recommendations to minimize the risk of injury to the patient was that the treating physician remain in the room with the patient throughout the procedure, carefully monitoring the positions of the urethral and rectal probes.
This recommendation was based on the then current labeling for the devices and remains unchanged today.
Laura Alonge
Issues Management Staff
240-276-3355
Subject: RE: Microwave Thermotherapy for Benign Prostatic Hyperplasia
Date: Wed, 27 Dec 2006 16:01:25 -0500
In October 2000, the FDA issued a Public Health Notification alerting clinicians to the possibility of serious, unanticipated adverse events associated with microwave thermotherapy for treatment of BPH ( http://www.fda.gov/cdrh/safety/bph.html ). One of the recommendations to minimize the risk of injury to the patient was that the treating physician remain in the room with the patient throughout the procedure, carefully monitoring the positions of the urethral and rectal probes.
This recommendation was based on the then current labeling for the devices and remains unchanged today.
Laura Alonge
Issues Management Staff
240-276-3355
FDA: Microwave Thermotherapy for Benign Prostatic Hyperplasia
From: "Alonge, Laura A."
Subject: RE: Microwave Thermotherapy for Benign Prostatic Hyperplasia
Date: Wed, 27 Dec 2006 16:01:25 -0500
In October 2000, the FDA issued a Public Health Notification alerting clinicians to the possibility of serious, unanticipated adverse events associated with microwave thermotherapy for treatment of BPH ( http://www.fda.gov/cdrh/safety/bph.html ). One of the recommendations to minimize the risk of injury to the patient was that the treating physician remain in the room with the patient throughout the procedure, carefully monitoring the positions of the urethral and rectal probes.
This recommendation was based on the then current labeling for the devices and remains unchanged today. (this is link to full article)
Laura Alonge
Issues Management Staff
240-276-3355
Subject: RE: Microwave Thermotherapy for Benign Prostatic Hyperplasia
Date: Wed, 27 Dec 2006 16:01:25 -0500
In October 2000, the FDA issued a Public Health Notification alerting clinicians to the possibility of serious, unanticipated adverse events associated with microwave thermotherapy for treatment of BPH ( http://www.fda.gov/cdrh/safety/bph.html ). One of the recommendations to minimize the risk of injury to the patient was that the treating physician remain in the room with the patient throughout the procedure, carefully monitoring the positions of the urethral and rectal probes.
This recommendation was based on the then current labeling for the devices and remains unchanged today. (this is link to full article)
Laura Alonge
Issues Management Staff
240-276-3355
FDA: Microwave Thermotherapy for Benign Prostatic Hyperplasia
From: "Alonge, Laura A."
Subject: RE: Microwave Thermotherapy for Benign Prostatic Hyperplasia
Date: Wed, 27 Dec 2006 16:01:25 -0500
In October 2000, the FDA issued a Public Health Notification alerting clinicians to the possibility of serious, unanticipated adverse events associated with microwave thermotherapy for treatment of BPH ( http://www.fda.gov/cdrh/safety/bph.html ). One of the recommendations to minimize the risk of injury to the patient was that the treating physician remain in the room with the patient throughout the procedure, carefully monitoring the positions of the urethral and rectal probes.
This recommendation was based on the then current labeling for the devices and remains unchanged today.
Laura Alonge
Issues Management Staff
240-276-3355
Subject: RE: Microwave Thermotherapy for Benign Prostatic Hyperplasia
Date: Wed, 27 Dec 2006 16:01:25 -0500
In October 2000, the FDA issued a Public Health Notification alerting clinicians to the possibility of serious, unanticipated adverse events associated with microwave thermotherapy for treatment of BPH ( http://www.fda.gov/cdrh/safety/bph.html ). One of the recommendations to minimize the risk of injury to the patient was that the treating physician remain in the room with the patient throughout the procedure, carefully monitoring the positions of the urethral and rectal probes.
This recommendation was based on the then current labeling for the devices and remains unchanged today.
Laura Alonge
Issues Management Staff
240-276-3355
Friday, December 15, 2006
TUMT catheter in place
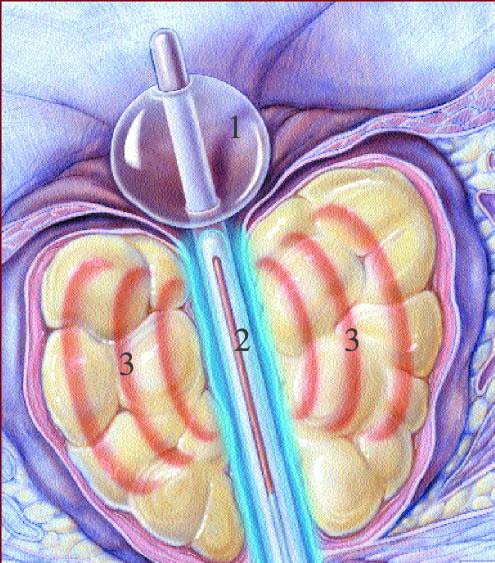
Cooled thermotherapy (TUMT)
catheter in place
1 = Balloon in urinary bladder, holding treatment catheter in place
2 = Microwave filament within prostatic urethra
3 = Microwaves radiating into prostatic adenoma
USRF Mission Statement
Urological Sciences Research Foundation, a California non-profit organization, was started in 1992 by the founder and current medical director, Leonard S. Marks, M.D. The primary mission of the foundation is as follows:To help advance the understanding of common urologic problems, increase the range of effective treatments for such conditions, and inform the medical and lay public of these problems and treatments.



Thursday, December 14, 2006
October 11, 2000 FDA health notification
FDA Public Health Notification: Serious Injuries from Microwave Thermotherapy for Benign Prostatic Hyperplasia
(You are encouraged to copy and distribute this information)
October 11, 2000
Dear Colleague:
This is to notify you of the potential for serious thermal injury and related complications associated with the use of microwave energy to treat benign prostatic hyperplasia (BPH), and to provide information that can help avoid these complications. Although the use of microwave thermotherapy for the treatment of BPH has been demonstrated to be safe and effective, and more than 25,000 procedures have been performed, we are concerned about some unexpected procedure-related complications that have occurred since the marketing of these devices.
Currently marketed devices include the Prostatron (Edap Technomed, Inc.) and the Targis System (Urologix, Inc.). Dornier Medical Systems, Inc. has received approval to market their UroWave System but is not yet marketing it. We are working with the manufacturers to ensure that labeling and training programs address these complications.
Nature of the Problem
Since 1996, we have received reports of 16 thermal injuries related to microwave thermotherapy systems. Of these, 10 resulted in fistula formation and 6 resulted in clinically significant tissue damage to the penis or urethra. These injuries may not be apparent at the time of treatment, and may take hours or days to develop. (Note that the original labeling for these devices did not list fistula formation as a procedure-related complication.) The reported injuries have required colostomies, partial amputation of the penis, and/or other therapeutic interventions.
We have identified several factors that may have contributed to the injuries noted:
* Incorrect placement or undetected migration of either the treatment catheter or the rectal temperature sensors;
* Failure of the physician to remain with the patient throughout the entire treatment duration;
* Failure to pause treatment when the patient is communicating serious pain;
* Oversedation of the patient, which compromises his ability to communicate pain;
* Treatment of patients who have undergone prior radiation therapy to the pelvic area;
* Treatment of patients whose prostate sizes are outside the ranges specified in the labeling; and
* Leakage from the balloons used to retain either the urethral catheter or the rectal temperature sensor in the correct anatomical position;
Recommendations
1. When considering a patient for microwave thermotherapy for BPH, ensure that he meets the device’s indications, including the criteria for eligible prostate size indicated for the specific system being used. Additionally, it is important to verify that the patient has not had prior radiation therapy to the pelvic area, as these patients are at increased risk of rectal fistula formation. Furthermore, the labeling of each device lists specific patient populations for which safety and effectiveness of this therapy are unknown (e.g., those with prostate cancer).
2. When discussing the procedure with the patient, it is important to ensure that he understands the risks and benefits listed in the labeling of the specific device. He should also understand the duration of the procedure, the level of pain or discomfort that should be considered normal, the importance of telling the physician of any unusual pain during treatment, how to operate any emergency stop button, and the need to remain as still as possible during treatment.
3. Carefully follow the instructions for use provided with these microwave systems. Note that they require the physician to continually supervise the procedure throughout the entire treatment period. The physician must (1) verify that the retention balloons of the urethral catheter and rectal temperature sensor probe are free of leaks, and (2) confirm the placement of the urethral catheter and rectal temperature sensor using acceptable methods (e.g., direct visualization, ultrasound imaging) both prior to treatment and other specified times consistent with the manufacturer’s recommendations. Either patient movement or component breakage may cause migration of a properly placed urethral catheter or rectal temperature sensor.
4. Be careful not to oversedate the patient. As patient perception of pain is an important safety mechanism to ensure that the heating of the tissue is not excessive, general or spinal anesthesia should not be used.
5. Closely monitor the patient and the equipment throughout the entire treatment, and manually pause treatment if the patient complains of excessive pain or anything unusual occurs.
Background
Microwave thermotherapy systems are intended to heat the prostate, resulting in the necrosis of periurethral prostatic tissue, to provide relief of urinary symptoms in patients with obstructive BPH. These devices heat the prostate to therapeutic levels using microwave energy delivered by an antenna contained within a specially designed urethral catheter. The catheter is designed so that when the balloon is seated at the neck of the bladder, the active portion of the antenna is positioned within the prostate. To prevent overheating, the systems circulate cooling fluid through the urethral catheter to protect the urethral tissue from excessive heat and automatically vary microwave energy output during treatment based on information supplied by temperature sensors placed posterior to the prostate within the rectum. Treatment may last from 30 to 60 minutes.
Because the catheter and/or the rectal temperature sensors can migrate during treatment, and because the correct placement of both of these components is critical for safe and effective treatment, the labeling for all these devices instructs the treating physician to: (1) verify that the urethral catheter (and rectal temperature sensor probe, if applicable) has a working retention balloon prior to placement, and (2) verify the proper position of both the urethral catheter and the rectal temperature sensors prior to and at specified time intervals consistent with the manufacturer’s recommendation for treatment. These requirements are intended to help ensure that catheter or rectal temperature sensor migration does not occur in a manner which would cause undetected excessive heating of surrounding tissues or the delivery of therapeutic heating levels to areas of the body that are not intended to receive treatment. The labeling for microwave thermotherapy devices also instructs the treating physician to monitor the equipment and patient during treatment, and manually reduce or pause the microwave power if the patient experiences excessive pain or extreme heating is observed.
Reporting Adverse Events to FDA
The Safe Medical Devices Act of 1990 (SMDA) requires hospitals and other user facilities to report deaths and serious injuries associated with the use of medical devices. FDA is interested in additional data on adverse events involving the use of microwave thermotherapy systems. When submitting a report, please identify the treatment protocol and catheter type, if known. Healthcare providers that are employed by facilities that are subject to FDA’s user facility reporting requirements should follow the reporting procedures established by their facilities. All other providers may submit their reports to MedWatch, FDA’s voluntary reporting program. The reports can be submitted by phone at 1-800-FDA-1088; by fax at 1-800-FDA-0178; by mail to MedWatch, Food and Drug Administration, HF-2, 5600 Fishers Lane, Rockville, Maryland 20857, or online at www.accessdata.fda.gov/scripts/medwatch.
Getting More Information
If you have questions regarding this letter, please contact the Issues Management Staff, Office of Surveillance and Biometrics (HFZ-510), 1350 Piccard Drive, Rockville, Maryland, 20850, by fax at 240-276-3356, or by e-mail at phann@cdrh.fda.gov. Additionally, a voice mail message may be left at 240-276-3357and your call will be returned as soon as possible.
All of the FDA medical device postmarket safety notifications can be found on the World Wide Web at http://www.fda.gov/cdrh/safety.html. Postmarket Safety notifications can also be obtained through e-mail on the day they are released by subscribing to our list server. Subscribe at: http://service.govdelivery.com/service/subscribe.html?code=USFDACDRH_10
Sincerely yours,
David W. Feigal, Jr., MD, MPH
Director
Center for Devices and Radiological Health
Food and Drug Administration
(You are encouraged to copy and distribute this information)
October 11, 2000
Dear Colleague:
This is to notify you of the potential for serious thermal injury and related complications associated with the use of microwave energy to treat benign prostatic hyperplasia (BPH), and to provide information that can help avoid these complications. Although the use of microwave thermotherapy for the treatment of BPH has been demonstrated to be safe and effective, and more than 25,000 procedures have been performed, we are concerned about some unexpected procedure-related complications that have occurred since the marketing of these devices.
Currently marketed devices include the Prostatron (Edap Technomed, Inc.) and the Targis System (Urologix, Inc.). Dornier Medical Systems, Inc. has received approval to market their UroWave System but is not yet marketing it. We are working with the manufacturers to ensure that labeling and training programs address these complications.
Nature of the Problem
Since 1996, we have received reports of 16 thermal injuries related to microwave thermotherapy systems. Of these, 10 resulted in fistula formation and 6 resulted in clinically significant tissue damage to the penis or urethra. These injuries may not be apparent at the time of treatment, and may take hours or days to develop. (Note that the original labeling for these devices did not list fistula formation as a procedure-related complication.) The reported injuries have required colostomies, partial amputation of the penis, and/or other therapeutic interventions.
We have identified several factors that may have contributed to the injuries noted:
* Incorrect placement or undetected migration of either the treatment catheter or the rectal temperature sensors;
* Failure of the physician to remain with the patient throughout the entire treatment duration;
* Failure to pause treatment when the patient is communicating serious pain;
* Oversedation of the patient, which compromises his ability to communicate pain;
* Treatment of patients who have undergone prior radiation therapy to the pelvic area;
* Treatment of patients whose prostate sizes are outside the ranges specified in the labeling; and
* Leakage from the balloons used to retain either the urethral catheter or the rectal temperature sensor in the correct anatomical position;
Recommendations
1. When considering a patient for microwave thermotherapy for BPH, ensure that he meets the device’s indications, including the criteria for eligible prostate size indicated for the specific system being used. Additionally, it is important to verify that the patient has not had prior radiation therapy to the pelvic area, as these patients are at increased risk of rectal fistula formation. Furthermore, the labeling of each device lists specific patient populations for which safety and effectiveness of this therapy are unknown (e.g., those with prostate cancer).
2. When discussing the procedure with the patient, it is important to ensure that he understands the risks and benefits listed in the labeling of the specific device. He should also understand the duration of the procedure, the level of pain or discomfort that should be considered normal, the importance of telling the physician of any unusual pain during treatment, how to operate any emergency stop button, and the need to remain as still as possible during treatment.
3. Carefully follow the instructions for use provided with these microwave systems. Note that they require the physician to continually supervise the procedure throughout the entire treatment period. The physician must (1) verify that the retention balloons of the urethral catheter and rectal temperature sensor probe are free of leaks, and (2) confirm the placement of the urethral catheter and rectal temperature sensor using acceptable methods (e.g., direct visualization, ultrasound imaging) both prior to treatment and other specified times consistent with the manufacturer’s recommendations. Either patient movement or component breakage may cause migration of a properly placed urethral catheter or rectal temperature sensor.
4. Be careful not to oversedate the patient. As patient perception of pain is an important safety mechanism to ensure that the heating of the tissue is not excessive, general or spinal anesthesia should not be used.
5. Closely monitor the patient and the equipment throughout the entire treatment, and manually pause treatment if the patient complains of excessive pain or anything unusual occurs.
Background
Microwave thermotherapy systems are intended to heat the prostate, resulting in the necrosis of periurethral prostatic tissue, to provide relief of urinary symptoms in patients with obstructive BPH. These devices heat the prostate to therapeutic levels using microwave energy delivered by an antenna contained within a specially designed urethral catheter. The catheter is designed so that when the balloon is seated at the neck of the bladder, the active portion of the antenna is positioned within the prostate. To prevent overheating, the systems circulate cooling fluid through the urethral catheter to protect the urethral tissue from excessive heat and automatically vary microwave energy output during treatment based on information supplied by temperature sensors placed posterior to the prostate within the rectum. Treatment may last from 30 to 60 minutes.
Because the catheter and/or the rectal temperature sensors can migrate during treatment, and because the correct placement of both of these components is critical for safe and effective treatment, the labeling for all these devices instructs the treating physician to: (1) verify that the urethral catheter (and rectal temperature sensor probe, if applicable) has a working retention balloon prior to placement, and (2) verify the proper position of both the urethral catheter and the rectal temperature sensors prior to and at specified time intervals consistent with the manufacturer’s recommendation for treatment. These requirements are intended to help ensure that catheter or rectal temperature sensor migration does not occur in a manner which would cause undetected excessive heating of surrounding tissues or the delivery of therapeutic heating levels to areas of the body that are not intended to receive treatment. The labeling for microwave thermotherapy devices also instructs the treating physician to monitor the equipment and patient during treatment, and manually reduce or pause the microwave power if the patient experiences excessive pain or extreme heating is observed.
Reporting Adverse Events to FDA
The Safe Medical Devices Act of 1990 (SMDA) requires hospitals and other user facilities to report deaths and serious injuries associated with the use of medical devices. FDA is interested in additional data on adverse events involving the use of microwave thermotherapy systems. When submitting a report, please identify the treatment protocol and catheter type, if known. Healthcare providers that are employed by facilities that are subject to FDA’s user facility reporting requirements should follow the reporting procedures established by their facilities. All other providers may submit their reports to MedWatch, FDA’s voluntary reporting program. The reports can be submitted by phone at 1-800-FDA-1088; by fax at 1-800-FDA-0178; by mail to MedWatch, Food and Drug Administration, HF-2, 5600 Fishers Lane, Rockville, Maryland 20857, or online at www.accessdata.fda.gov/scripts/medwatch.
Getting More Information
If you have questions regarding this letter, please contact the Issues Management Staff, Office of Surveillance and Biometrics (HFZ-510), 1350 Piccard Drive, Rockville, Maryland, 20850, by fax at 240-276-3356, or by e-mail at phann@cdrh.fda.gov. Additionally, a voice mail message may be left at 240-276-3357and your call will be returned as soon as possible.
All of the FDA medical device postmarket safety notifications can be found on the World Wide Web at http://www.fda.gov/cdrh/safety.html. Postmarket Safety notifications can also be obtained through e-mail on the day they are released by subscribing to our list server. Subscribe at: http://service.govdelivery.com/service/subscribe.html?code=USFDACDRH_10
Sincerely yours,
David W. Feigal, Jr., MD, MPH
Director
Center for Devices and Radiological Health
Food and Drug Administration
Urologix TUMT Physician Locator
Physician Locator
For a list of urologists in your area who treat with Cooled ThermoTherapy™, please call customer service at 888-229-0772 or send an email to us by clicking here.
Urologix provides this information solely as a convenience and not as an endorsement or recommendation of any treating urologist.
For a list of urologists in your area who treat with Cooled ThermoTherapy™, please call customer service at 888-229-0772 or send an email to us by clicking here.
Urologix provides this information solely as a convenience and not as an endorsement or recommendation of any treating urologist.
TUMT serious injuries and complications
How Well It Works
http://www.sjmercyhealth.org/body.cfm?id=431&action=detail&aeproductid=HW_Catholic&aearticleid=ug1939
Studies note that TUMT is more effective than treatment with the alpha-blocker terazosin when checked 18 months later.1
In one study, transurethral resection of the prostate (TURP) improved symptoms better than TUMT. But in two other studies, there was no major difference in how well the two treatments worked.1
Risks
The main complication of TUMT is the inability to urinate (urinary retention) for more than a week.2 This condition is treated by inserting a tube directly through the abdominal wall into the bladder to drain urine (suprapubic catheter). Erection problems and retrograde ejaculation (ejaculation backward into the bladder) appear to be less common after TUMT than after TURP.2
Other complications include persistent irritation of the urethra and blood in the urine.1
Recent reports have warned that the procedure has in a small number of cases caused serious injuries and complications, including damage to the penis and urethra. Injuries have required colostomies, partial amputation of the penis, and other procedures. In December 2000, the U.S. Food and Drug Administration (FDA) issued a warning about these injuries.3
http://www.sjmercyhealth.org/body.cfm?id=431&action=detail&aeproductid=HW_Catholic&aearticleid=ug1939
Studies note that TUMT is more effective than treatment with the alpha-blocker terazosin when checked 18 months later.1
In one study, transurethral resection of the prostate (TURP) improved symptoms better than TUMT. But in two other studies, there was no major difference in how well the two treatments worked.1
Risks
The main complication of TUMT is the inability to urinate (urinary retention) for more than a week.2 This condition is treated by inserting a tube directly through the abdominal wall into the bladder to drain urine (suprapubic catheter). Erection problems and retrograde ejaculation (ejaculation backward into the bladder) appear to be less common after TUMT than after TURP.2
Other complications include persistent irritation of the urethra and blood in the urine.1
Recent reports have warned that the procedure has in a small number of cases caused serious injuries and complications, including damage to the penis and urethra. Injuries have required colostomies, partial amputation of the penis, and other procedures. In December 2000, the U.S. Food and Drug Administration (FDA) issued a warning about these injuries.3
Technological Advances in Adult Urology
Surgical, Pharmacological, and Technological Advances in Adult and Pediatric Urology: "One of the primary concerns of TUMT is the durability of symptom improvement. The long-term outcomes data are inconsistent."
Transurethral microwave thermotherapy (TUMT).
Transurethral microwave thermotherapy (TUMT). Uses microwaves sent through a catheter to heat and destroy excess prostate tissue. For most TUMT devices, a cooling system protects the portion of the urethra that goes through the prostate during the procedure.
The TUMT procedure takes about one hour and can be an option for men who should not have major surgery because they have other medical problems. Microwave therapy does not cure BPH, but it reduces urinary frequency, urgency, straining, and intermittent flow. It does not completely correct the problem of incomplete emptying of the bladder.
TUMT has limited long-term effects. Up to 40 percent of men treated may need re-treatment a few years later. Though rare, there have been cases reported of incontinence and impotence with this procedure.
Although microwave thermotherapy has been demonstrated to be safe and effective, the FDA has been concerned in the past about unexpected procedure-related complications that occurred since these devices were marketed.
http://www.fda.gov/fdac/features/2006/306_prostate.html
The TUMT procedure takes about one hour and can be an option for men who should not have major surgery because they have other medical problems. Microwave therapy does not cure BPH, but it reduces urinary frequency, urgency, straining, and intermittent flow. It does not completely correct the problem of incomplete emptying of the bladder.
TUMT has limited long-term effects. Up to 40 percent of men treated may need re-treatment a few years later. Though rare, there have been cases reported of incontinence and impotence with this procedure.
Although microwave thermotherapy has been demonstrated to be safe and effective, the FDA has been concerned in the past about unexpected procedure-related complications that occurred since these devices were marketed.
http://www.fda.gov/fdac/features/2006/306_prostate.html
Prostate Health: What Every Man Needs to Know
Prostate Health: What Every Man Needs to Know:
"Transurethral microwave thermotherapy (TUMT). Uses microwaves sent through a catheter to heat and destroy excess prostate tissue. For most TUMT devices, a cooling system protects the portion of the urethra that goes through the prostate during the procedure. The TUMT procedure takes about one hour and can be an option for men who should not have major surgery because they have other medical problems.
Microwave therapy does not cure BPH, but it reduces urinary frequency, urgency, straining, and intermittent flow. It does not completely correct the problem of incomplete emptying of the bladder. TUMT has limited long-term effects. Up to 40 percent of men treated may need re-treatment a few years later.
Though rare, there have been cases reported of incontinence and impotence with this procedure. Although microwave thermotherapy has been demonstrated to be safe and effective, the FDA has been concerned in the past about unexpected procedure-related complications that occurred since these devices were marketed."
"Transurethral microwave thermotherapy (TUMT). Uses microwaves sent through a catheter to heat and destroy excess prostate tissue. For most TUMT devices, a cooling system protects the portion of the urethra that goes through the prostate during the procedure. The TUMT procedure takes about one hour and can be an option for men who should not have major surgery because they have other medical problems.
Microwave therapy does not cure BPH, but it reduces urinary frequency, urgency, straining, and intermittent flow. It does not completely correct the problem of incomplete emptying of the bladder. TUMT has limited long-term effects. Up to 40 percent of men treated may need re-treatment a few years later.
Though rare, there have been cases reported of incontinence and impotence with this procedure. Although microwave thermotherapy has been demonstrated to be safe and effective, the FDA has been concerned in the past about unexpected procedure-related complications that occurred since these devices were marketed."
TUMT 2000 article
http://www.yourpatienteducation.com/PatientPortal/Public/ArticlePromoted.aspx?ArticleID=HW5ug1939: "How Well It Works
Studies note that TUMT is more effective than treatment with the alpha-blocker terazosin when checked 18 months later.1
In one study, transurethral resection of the prostate (TURP) improved symptoms better than TUMT. But in two other studies, there was no major difference in how well the two treatments worked.1
Risks
The main complication of TUMT is the inability to urinate (urinary retention) for more than a week.2 This condition is treated by inserting a tube directly through the abdominal wall into the bladder to drain urine (suprapubic catheter). Erection problems and retrograde ejaculation (ejaculation backward into the bladder) appear to be less common after TUMT than after TURP.2
Other complications include persistent irritation of the urethra and blood in the urine.1
Recent reports have warned that the procedure has in a small number of cases caused serious injuries and complications, including damage to the penis and urethra. Injuries have required colostomies, partial amputation of the penis, and other procedures. In December 2000, the U.S. Food and Drug Administration (FDA) issued a warning about these injuries.3"
Studies note that TUMT is more effective than treatment with the alpha-blocker terazosin when checked 18 months later.1
In one study, transurethral resection of the prostate (TURP) improved symptoms better than TUMT. But in two other studies, there was no major difference in how well the two treatments worked.1
Risks
The main complication of TUMT is the inability to urinate (urinary retention) for more than a week.2 This condition is treated by inserting a tube directly through the abdominal wall into the bladder to drain urine (suprapubic catheter). Erection problems and retrograde ejaculation (ejaculation backward into the bladder) appear to be less common after TUMT than after TURP.2
Other complications include persistent irritation of the urethra and blood in the urine.1
Recent reports have warned that the procedure has in a small number of cases caused serious injuries and complications, including damage to the penis and urethra. Injuries have required colostomies, partial amputation of the penis, and other procedures. In December 2000, the U.S. Food and Drug Administration (FDA) issued a warning about these injuries.3"
FDA warning Microwave therapy warning. JAMA, 284(21): 2711.
Recent reports have warned that the procedure has in a small number of cases caused serious injuries and complications, including damage to the penis and urethra. Injuries have required colostomies, partial amputation of the penis, and other procedures. In December 2000, the U.S. Food and Drug Administration (FDA) issued a warning on these injuries. 3
http://health.yahoo.com/topic/men/treatment/article/healthwise/ug1939
http://www.webmd.com/hw/mens_conditions/ug1939.asp#ug1908
U.S. Food and Drug Administration (2002). Microwave therapy warning. JAMA, 284(21): 2711.
http://health.yahoo.com/topic/men/treatment/article/healthwise/ug1939
http://www.webmd.com/hw/mens_conditions/ug1939.asp#ug1908
TUMT bladder neck trauma
sense of urinary urgency. However, only 5% of patients reported their pain as being severe during Targis therapy. Despite this, more than one half of these patients required substantial oral analgesics during treatment. Higher energy protocols appear to have a slightly higher level of initial pain due to the initial higher power, which appears to resolve and return to the same level of comfort as the lower-energy protocols soon into treatment.
Reports of complications vary, and range from 0 to 38%, based on the study and the investigators' criteria for complications. For example, Ohigashi et al. reported no serious side-effects in 91 patients treated with low-power over 5-year followup (25). Others report complications including acute urinary incontinence, urinary tract infection, and urinary retention. The risk for urinary tract infections rises with each day of catheterization. In addition, the necrotic tissue that remains in the prostatic fossa after TUMT may increase the risk of colonization and infection. Treatment morbidity of higher energy protocols is moderate and consists mainly of the need for catheterization and a higher percentage of retrograde ejaculation (17).
Erectile dysfunction after TUMT is rare if a patient is previously normal, but is commonly observed in patients with prior erectile difficulties. Although causes have not been fully elucidated, psychogenic factors, bladder neck trauma, and neurogenic voiding dysfunction probably play a role. Lower-energy TUMT protocols have a lower incidence of erectile dysfunction compared to higher-energy protocols but at the expense of better urinary results. Francisca et al. (43) reported no change in sexual performance after low-energy TUMT when compared to a sham procedure in 147 patients.
A variety of other rare but reported complications following TUMT occur. This includes, but is not limited to, urethrorectal fistula (44), bladder perforation, and improper catheter placement. An emphysematous prostatic abscess (45) has been reported after low-energy TUMT in a 55-year old man with diabetes mellitus and cirrhosis. Proper intratreatment physician and nursing observation are vital to decrease these risks.
Reports of complications vary, and range from 0 to 38%, based on the study and the investigators' criteria for complications. For example, Ohigashi et al. reported no serious side-effects in 91 patients treated with low-power over 5-year followup (25). Others report complications including acute urinary incontinence, urinary tract infection, and urinary retention. The risk for urinary tract infections rises with each day of catheterization. In addition, the necrotic tissue that remains in the prostatic fossa after TUMT may increase the risk of colonization and infection. Treatment morbidity of higher energy protocols is moderate and consists mainly of the need for catheterization and a higher percentage of retrograde ejaculation (17).
Erectile dysfunction after TUMT is rare if a patient is previously normal, but is commonly observed in patients with prior erectile difficulties. Although causes have not been fully elucidated, psychogenic factors, bladder neck trauma, and neurogenic voiding dysfunction probably play a role. Lower-energy TUMT protocols have a lower incidence of erectile dysfunction compared to higher-energy protocols but at the expense of better urinary results. Francisca et al. (43) reported no change in sexual performance after low-energy TUMT when compared to a sham procedure in 147 patients.
A variety of other rare but reported complications following TUMT occur. This includes, but is not limited to, urethrorectal fistula (44), bladder perforation, and improper catheter placement. An emphysematous prostatic abscess (45) has been reported after low-energy TUMT in a 55-year old man with diabetes mellitus and cirrhosis. Proper intratreatment physician and nursing observation are vital to decrease these risks.
increase anesthetic risk, increased risk for secondary procedures, and risk for bleeding.
TUMT in patients in urinary retention Because patients presenting with urinary retention generally are older, have a larger prostate volume, and have more renal insufficiency, they are at increase anesthetic risk, increased risk for secondary procedures, and risk for bleeding. In the past, TUMT was thought to be contraindicated because of a high failure rate.
However, with the advent of high-energy TUMT, patients are now offered this less-invasive therapy. Djavan et al. reported a 94% success rate at 12 weeks in 31 patients presenting in retention (40), although the 1-year retreatment rate is estimated to be 25% (41). Schelin reported that 80% of their cohort was relieved of an indwelling catheter after TUMT, and those who failed all had large median lobes or protruding lateral lobes into the bladder (42). Robinette et al. (18) reported that 44 of 60 patients in retention were able to void spontaneously at 6 months after therapy with the Prostatron 2.0 or 2.5, as were 32 of 35 followed at 12 months.
COMPLICATIONS During the procedure, patients commonly experience mild perineal warmth, mild pain,
However, with the advent of high-energy TUMT, patients are now offered this less-invasive therapy. Djavan et al. reported a 94% success rate at 12 weeks in 31 patients presenting in retention (40), although the 1-year retreatment rate is estimated to be 25% (41). Schelin reported that 80% of their cohort was relieved of an indwelling catheter after TUMT, and those who failed all had large median lobes or protruding lateral lobes into the bladder (42). Robinette et al. (18) reported that 44 of 60 patients in retention were able to void spontaneously at 6 months after therapy with the Prostatron 2.0 or 2.5, as were 32 of 35 followed at 12 months.
COMPLICATIONS During the procedure, patients commonly experience mild perineal warmth, mild pain,
TUMT CONTRAINDICATIONS
CONTRAINDICATIONS
All patients undergoing transurethral procedures must have a documented sterile urine culture and must be evaluated for prostate or urothelial cancer if clinically suspected. Patients with neurogenic bladder voiding dysfunction should have their underlying neurogenic problem evaluated and treated. Contraindications specific to TUMT are evolving as the technology changes and outcomes are studied further. Patients with a history of TURP or pelvic trauma should not undergo TUMT because of potential alterations in pelvic anatomy. Patients with glands that are smaller than 25 gm. or a prostatic urethral length of less than 3 cm respond poorly to TUMT, as do patients with glands greater than 100 gm or patients with a prominent median bar.
Other contraindications include patients with penile prosthesis, severe urethral stricture disease, Leriche syndrome/severe peripheral vascular disease, or an artificial urinary sphincter. Patients with pacemakers and defibrillators need clearance from their cardiologist concerning turning their pacemakers off during therapy.
Hip replacement is no longer a contraindication. Acute urinary retention was previously thought to be a contraindication to TUMT; however, high-energy TUMT has shown to be promising in this population, although efficacy has yet to be determined
All patients undergoing transurethral procedures must have a documented sterile urine culture and must be evaluated for prostate or urothelial cancer if clinically suspected. Patients with neurogenic bladder voiding dysfunction should have their underlying neurogenic problem evaluated and treated. Contraindications specific to TUMT are evolving as the technology changes and outcomes are studied further. Patients with a history of TURP or pelvic trauma should not undergo TUMT because of potential alterations in pelvic anatomy. Patients with glands that are smaller than 25 gm. or a prostatic urethral length of less than 3 cm respond poorly to TUMT, as do patients with glands greater than 100 gm or patients with a prominent median bar.
Other contraindications include patients with penile prosthesis, severe urethral stricture disease, Leriche syndrome/severe peripheral vascular disease, or an artificial urinary sphincter. Patients with pacemakers and defibrillators need clearance from their cardiologist concerning turning their pacemakers off during therapy.
Hip replacement is no longer a contraindication. Acute urinary retention was previously thought to be a contraindication to TUMT; however, high-energy TUMT has shown to be promising in this population, although efficacy has yet to be determined
Transurethral Microwave Thermotherapy (TUMT) | MAC Jurisdiction 3 | Noridianmedicare.com
Transurethral Microwave Thermotherapy (TUMT) | MAC Jurisdiction 3 | Noridianmedicare.com: "TUMT, an appropriate therapy for symptomatic benign prostatic hypertrophy (BPH), is a method of delivering microwave heating sufficient to destroy prostatic adenoma tissue without significant damage to surrounding tissue. The FDA has, on May 3, 1996, approved a device for delivering this microwave therapy. TUMT is another nonsurgical therapy for BPH, and is appropriate when the following indications are met.
Indications:
All of the following characteristics must be present.
A. Bladder Outlet Obstruction (BOO) and Lower Urinary Tract Symptoms (LUTS) of significant degree to cause an American Urological Association Symptom Score above seven. A score from 0-7 reflects mild symptoms, from 8-19 moderate, and from 20-35 severe. A patient with mild symptoms may be treated with medicine or, appropriately, receive no treatment at all. A patient with moderate symptoms may be treated with medical or surgical procedures. Noridian leaves this decision to the physician and the patient.
B. A peak urine flow rate of 15 milliliters per second or less on a voided volume of 125 milliliters or greater.
Relative contraindications:
A. Prostate cancer
B. Neurogenic bladder
C. Active urinary tract infection
D. Active cystolithiasis
E. Gross hematuria
F. Urethral stricture
G. Bladder neck contracture
H. Acute prostatitis
I. Cardiac pacemaker
When present, active cystolithiasis or active infection should be treated prior to treatment with TUMT.
When prostate cancer and urinary obstruction are both present, TUMT may be appropriate therapy for relief of the urinary obstruction.
Absolute contraindication:
The presence of a metallic hip replacement."
Indications:
All of the following characteristics must be present.
A. Bladder Outlet Obstruction (BOO) and Lower Urinary Tract Symptoms (LUTS) of significant degree to cause an American Urological Association Symptom Score above seven. A score from 0-7 reflects mild symptoms, from 8-19 moderate, and from 20-35 severe. A patient with mild symptoms may be treated with medicine or, appropriately, receive no treatment at all. A patient with moderate symptoms may be treated with medical or surgical procedures. Noridian leaves this decision to the physician and the patient.
B. A peak urine flow rate of 15 milliliters per second or less on a voided volume of 125 milliliters or greater.
Relative contraindications:
A. Prostate cancer
B. Neurogenic bladder
C. Active urinary tract infection
D. Active cystolithiasis
E. Gross hematuria
F. Urethral stricture
G. Bladder neck contracture
H. Acute prostatitis
I. Cardiac pacemaker
When present, active cystolithiasis or active infection should be treated prior to treatment with TUMT.
When prostate cancer and urinary obstruction are both present, TUMT may be appropriate therapy for relief of the urinary obstruction.
Absolute contraindication:
The presence of a metallic hip replacement."
Minimally invasive treatment for BPH
- Transurethral incision of the prostate (TUIP) has actually been in use for many years and, for a long time, was the only alternative to TURP. It may be performed with local anesthesia and sedation.
- TUIP is suitable for patients with small prostates and for patients unlikely to tolerate TURP well because of other medical conditions.
- TUIP is associated with less bleeding and fluid absorption compared to TURP. It is also associated with a lower incidence of retrograde ejaculation and impotence compared to TURP.
- Lasers deliver heat to the prostate in a variety of ways.
- They may be used to directly evaporate, ie, melt away prostate tissue. They may also be used in a manner in which the laser is not actually in direct contact with the prostate but delivers heat energy into the prostate, resulting in cell death of the prostate tissue. Laser fibers may first be placed directly into the prostate tissue and then turned on, releasing energy into the tissue. All these laser treatments essentially cause thermal destruction of prostate tissue (coagulation necrosis). Over time, this destroyed tissue then contracts, with resultant decreased prostatic volume.
- Lasers may be used in a knifelike fashion to directly cut away prostate tissue, similar to a TURP procedure.
- Laser treatment usually results in decreased bleeding, fluid absorption, length of hospital stay, and incidence of impotence and retrograde ejaculation when compared to standard TURP; however, in patients in whom lasers are used for thermal destruction (coagulation necrosis), they may cause significant swelling of the prostate, resulting in prolonged catheterization after the procedure. Additionally, because treating tissue with a laser involves a time interval during which dead cells slough and healing follows, patients may experience urinary urgency or an irritation, resulting in frequent or uncomfortable urination for some weeks.
- The results of laser therapy are variable in that many lasers are being used in many different ways. They usually bring about more relief of urinary symptoms than treatment with medicines, but not quite as much as provided by a TURP procedure.
- A laser treatment in which the laser is used to excise prostate tissue like a knife (in a fashion similar to TURP) has recently been shown to be as effective as TURP.
- The use of microwave energy, termed transurethral microwave therapy (TUMT), delivers heat to the prostate via a urethral catheter or a transrectal route.
- The surface closest to the probe (the rectal or urethral surface) is cooled to prevent injury. The heat causes cell death, with subsequent tissue contraction, thereby decreasing prostatic volume.
- TUMT can be performed in the outpatient setting with local anesthesia.
- Microwave treatment appears to be associated with significant prostatic swelling; a considerable number of patients require replacement of a urinary catheter until the swelling somewhat subsides. In terms of efficacy, TUMT places between medical therapy and TURP.
- Transurethral needle ablation of the prostate (TUNA) involves using high-frequency radio waves to produce heat, resulting in a similar process of thermal injury to the prostate as previously described. A specially designed transurethral device with needles is used to deliver the energy.
- TUNA can be performed under local anesthesia, allowing the patient to go home the same day.
- Similar to microwave treatment, radiofrequency treatment is quite popular, and a number of urologists have experience with its use.
- Radiofrequency treatment appears to reliably result in significant relief of symptoms and better urine flow, although not quite to the extent achieved with TURP.
- High-intensity ultrasound energy therapy delivers heat to prostate tissue, with the subsequent process of thermal injury.
- High-intensity ultrasound waves may be delivered rectally or extracorporeally and can be used with the patient on intravenous sedation.
- Urinary retention appears to be common with its use.
- High-intensity ultrasound energy also produces moderate results in terms of improvement of the urinary flow rate and urinary symptoms, although its use is now relatively limited compared to the more popular TUNA and TUMT.
- Water-induced thermotherapy is a relatively new procedure in which heated water is circulated through a balloon in the prostatic urethra, thus initiating a process of thermal destruction of prostate tissue.
- Mechanical approaches are used less commonly and are usually reserved for patients who cannot have a formal surgical procedure. Mechanical approaches do not involve the use of energy to treat the prostate.
- Prostatic stents are flexible devices that can expand when put in place to improve the flow of urine past the prostate. Their use has been associated with encrustation, pain, incontinence, and overgrowth of tissue through the stent, possibly making their removal quite difficult. To date, their full role and long-term effects are not fully known.
- Balloon dilation involves transurethral placement of a balloon, which is then inflated with the intent of expanding the prostatic urethra. Balloon dilation has largely been abandoned. Efficacy has not been demonstrated with this procedure.
Endotext.com - BENIGN PROSTATE DISORDERS
Endotext.com - BENIGN PROSTATE DISORDERS: "Other Minimally Invasive Therapies
Thermoablation is the principle underlying the remaining minimally invasive available treatments that have been introduced thus far174 and these include transurethral microwave thermotherapy and transurethral electrovaporization of the prostate.
In a study of 200 patients undergoing transurethral microwave thermotherapy (TUMT), a good initial response was achieved in 80% of patients175. However, 22% of patients in this study required re-treatment with conventional methods and there was a significant complication rate reported. As such it is a second line option only at this stage176. In a further study of high energy TUMT versus TURP, the IPSS improved in the TUMT group by 60% in year 1 however by 3 years, the improvement was not as apparent, being only 43% on IPSS.. Again, the re-treatment rate was 20% at 3 years. Voiding flow rate as measured by uroflowmetry improved by 64% at year 1, but this reduced to 29% by the end of year 3. This may be compared to the �gold-standard� TURP which had an IPSS reduction of 80-85% that remained stable over the 3 years, with a re-treatment rate of only 13%. Voiding flow rates improved by 214% in the TURP group and remained stable whilst re-treatments were generally for complications (eg. strictures or bladder neck contractures) rather than treatment failures177. Note that with lower energy TUMT protocols there is much less improvement in IPSS scores and voiding flow rates, and with 50-60% pre-treatment rates178.
Transurethral electrovaporization of the prostate (TUVT) has had promising results. In a study of 235 men randomised to TURP or TUVT, both groups achieved IPSS reductions of around 12 points and improvements in Qmax of 10ml/sec179. However, TUVT did not lead to a reduction in postoperative morbidity or shorter hospital stays."
Thermoablation is the principle underlying the remaining minimally invasive available treatments that have been introduced thus far174 and these include transurethral microwave thermotherapy and transurethral electrovaporization of the prostate.
In a study of 200 patients undergoing transurethral microwave thermotherapy (TUMT), a good initial response was achieved in 80% of patients175. However, 22% of patients in this study required re-treatment with conventional methods and there was a significant complication rate reported. As such it is a second line option only at this stage176. In a further study of high energy TUMT versus TURP, the IPSS improved in the TUMT group by 60% in year 1 however by 3 years, the improvement was not as apparent, being only 43% on IPSS.. Again, the re-treatment rate was 20% at 3 years. Voiding flow rate as measured by uroflowmetry improved by 64% at year 1, but this reduced to 29% by the end of year 3. This may be compared to the �gold-standard� TURP which had an IPSS reduction of 80-85% that remained stable over the 3 years, with a re-treatment rate of only 13%. Voiding flow rates improved by 214% in the TURP group and remained stable whilst re-treatments were generally for complications (eg. strictures or bladder neck contractures) rather than treatment failures177. Note that with lower energy TUMT protocols there is much less improvement in IPSS scores and voiding flow rates, and with 50-60% pre-treatment rates178.
Transurethral electrovaporization of the prostate (TUVT) has had promising results. In a study of 235 men randomised to TURP or TUVT, both groups achieved IPSS reductions of around 12 points and improvements in Qmax of 10ml/sec179. However, TUVT did not lead to a reduction in postoperative morbidity or shorter hospital stays."
contraindications for ProlieveTM TUMT
III. CONTRAINDICATIONS
The contraindications for ProlieveTM are:
· Patients whose pain response has been significantly decreased by any means (previous
surgery, regional or local anesthetic, or other relevant condition which is determined
by the physician upon evaluation) because the patients' ability to detect pain is a
treatment safety mechanism.
* Severe urethral stricture preventing catheterization.
· Current urinary or prostatic infection.
Presence of a penile or urinary sphincter implant.
· Prostate size <20g>80g.
· Peripheral arterial disease with intermittent claudication or Leriches Syndrome (i.e.,
claudication of the buttocks or perineum).
PMA P030006: SSED page 1 of 15
Protruding median lobe resulting in a "ball-valve" type of obstruction at the bladder
neck.
* Evidence of prostatic cancer or bladder cancer.
• Presence of metallic implants, e.g. pelvic, femur, penile prosthesis, etc.
Presence of implanted cardiac pacemakers, or defibrillators.
* Previous transurethral prostatectomy.
* Patients interested in the preservation of future fertility.
* Patients with a previous history of pelvic radiation.
* Patients with coagulation disorders.
* Patients with renal impairment.
* Patients with neurological disorders that might affect bladder function.
* Patients with bladder stones and large post voiding residual (greater than 250 mL).
The contraindications for ProlieveTM are:
· Patients whose pain response has been significantly decreased by any means (previous
surgery, regional or local anesthetic, or other relevant condition which is determined
by the physician upon evaluation) because the patients' ability to detect pain is a
treatment safety mechanism.
* Severe urethral stricture preventing catheterization.
· Current urinary or prostatic infection.
Presence of a penile or urinary sphincter implant.
· Prostate size <20g>80g.
· Peripheral arterial disease with intermittent claudication or Leriches Syndrome (i.e.,
claudication of the buttocks or perineum).
PMA P030006: SSED page 1 of 15
Protruding median lobe resulting in a "ball-valve" type of obstruction at the bladder
neck.
* Evidence of prostatic cancer or bladder cancer.
• Presence of metallic implants, e.g. pelvic, femur, penile prosthesis, etc.
Presence of implanted cardiac pacemakers, or defibrillators.
* Previous transurethral prostatectomy.
* Patients interested in the preservation of future fertility.
* Patients with a previous history of pelvic radiation.
* Patients with coagulation disorders.
* Patients with renal impairment.
* Patients with neurological disorders that might affect bladder function.
* Patients with bladder stones and large post voiding residual (greater than 250 mL).
Hyperthermia, Induced, contraindications
Hyperthermia, Induced, contraindications: "J Urol. 1992 Aug ;148:321-5 [Pubmed] [Scholar] [Select] [Drop] [Hide] [Show]
Transrectal microwave hyperthermia for benign prostatic hyperplasia: long-term clinical, pathological and ultrastructural patterns.
F Montorsi, L Galli, G Guazzoni, R Colombo, G Bulfamante, L Barbieri, V Matozzo, V Grazioli, P Rigatti
Transrectal microwave hyperthermia of the prostate was administered to 191 patients with bladder outlet obstruction due to benign prostatic hyperplasia who were either at poor operative risk or who refused surgery. Patients were divided in 2 groups according to age and they underwent either 5 or 10, 60-minute sessions of hyperthermia, with a calculated intraprostatic temperature of 42.5 plus or minus 0.5C. Light and electron microscopy showed no irreversible damage at the glandular epithelium but did demonstrate a significant increase in neoformed intraprostatic capillary-like vessels. At 1, 12 and 24 months residual urine volume was significantly decreased in the majority of patients but only a minor amelioration of urinary flow rates and subjective symptoms was observed. According to maximum flow nomograms all patients were still obstructed postoperatively. Transrectal hyperthermia cannot be considered a genuine alternative to surgery for patients with bladder outlet obstruction due to benign prostatic hyperplasia."
Transrectal microwave hyperthermia for benign prostatic hyperplasia: long-term clinical, pathological and ultrastructural patterns.
F Montorsi, L Galli, G Guazzoni, R Colombo, G Bulfamante, L Barbieri, V Matozzo, V Grazioli, P Rigatti
Transrectal microwave hyperthermia of the prostate was administered to 191 patients with bladder outlet obstruction due to benign prostatic hyperplasia who were either at poor operative risk or who refused surgery. Patients were divided in 2 groups according to age and they underwent either 5 or 10, 60-minute sessions of hyperthermia, with a calculated intraprostatic temperature of 42.5 plus or minus 0.5C. Light and electron microscopy showed no irreversible damage at the glandular epithelium but did demonstrate a significant increase in neoformed intraprostatic capillary-like vessels. At 1, 12 and 24 months residual urine volume was significantly decreased in the majority of patients but only a minor amelioration of urinary flow rates and subjective symptoms was observed. According to maximum flow nomograms all patients were still obstructed postoperatively. Transrectal hyperthermia cannot be considered a genuine alternative to surgery for patients with bladder outlet obstruction due to benign prostatic hyperplasia."
eMedicine - Transurethral Microwave Thermotherapy of the Prostate (TUMT) : Article by Jonathan Rubenstein, MD
eMedicine - Transurethral Microwave Thermotherapy of the Prostate (TUMT) : Article by Jonathan Rubenstein, MD: "Contraindications: Several general contraindications to all prostatic surgeries exist, such as active urinary infection or known or suspected prostate or urothelial cancer. Consider each of these before a treatment plan is instituted. Patients with neurogenic bladder voiding dysfunction should have their underlying neurogenic problem evaluated and treated.
Contraindications specific to TUMT are evolving as the technology changes and outcomes are studied further. Patients with a history of TURP or pelvic trauma should not undergo TUMT because of potential alterations in pelvic anatomy. Patients with glands that are smaller than 30 g or a prostatic urethral length of less than 3 cm respond poorly to TUMT, as do patients with glands greater than 100 g and patients with a prominent median bar.
Other contraindications include patients with metallic implants, penile prosthesis, severe urethral stricture disease, Leriche syndrome and/or severe peripheral vascular disease, or an artificial urinary sphincter. Patients with pacemakers need clearance from their cardiologists concerning turning their pacemakers off during therapy, although performing TUMT in this group should be approached with apprehension.
Hip replacement is no longer a contraindication. Acute urinary retention previously was thought to be a contraindication to TUMT. However, high-energy TUMT has shown promising results in this population, although efficacy has yet to be determined. Patients presenting in retention tend to be ill, with greater comorbidities; thus, they might benefit from the less invasive nature of TUMT."
Contraindications specific to TUMT are evolving as the technology changes and outcomes are studied further. Patients with a history of TURP or pelvic trauma should not undergo TUMT because of potential alterations in pelvic anatomy. Patients with glands that are smaller than 30 g or a prostatic urethral length of less than 3 cm respond poorly to TUMT, as do patients with glands greater than 100 g and patients with a prominent median bar.
Other contraindications include patients with metallic implants, penile prosthesis, severe urethral stricture disease, Leriche syndrome and/or severe peripheral vascular disease, or an artificial urinary sphincter. Patients with pacemakers need clearance from their cardiologists concerning turning their pacemakers off during therapy, although performing TUMT in this group should be approached with apprehension.
Hip replacement is no longer a contraindication. Acute urinary retention previously was thought to be a contraindication to TUMT. However, high-energy TUMT has shown promising results in this population, although efficacy has yet to be determined. Patients presenting in retention tend to be ill, with greater comorbidities; thus, they might benefit from the less invasive nature of TUMT."
eMedicine - Transurethral Microwave Thermotherapy of the Prostate (TUMT) : Article by Jonathan Rubenstein, MD
eMedicine - Transurethral Microwave Thermotherapy of the Prostate (TUMT) : Article by Jonathan Rubenstein, MD: "RELEVANT ANATOMY AND CONTRAINDICATIONS Section 4 of 11 Click here to go to the previous section in this topic Click here to go to the top of this page Click here to go to the next section in this topic
Author Information Introduction Indications Relevant Anatomy And Contraindications Workup Treatment Complications Outcome And Prognosis Future And Controversies Pictures Bibliography
Relevant Anatomy: The urinary bladder is derived embryologically from the urogenital sinus. The detrusor musculature makes up the bulk of the bladder and is stimulated mainly by the parasympathetic nervous system. The ureters enter the bladder at the corners of the trigone. The prostate, which originates from the mesenchyme surrounding the urogenital sinus, is a compound tubuloalveolar gland whose base abuts the bladder neck and whose apex merges with the membranous urethra at the urogenital diaphragm. The normal adult gland is cone-shaped and is 4.4 cm in transverse diameter across the base, 3.4 cm in length, and 2.6 cm in anteroposterior direction. Its blood supply is from the prostatovesicular artery, a branch of the inferior vesical artery from the hypogastric artery.
The nerve supply is from the pelvic plexus, which travels with the prostatovesicular artery. Alpha-adrenergic nerves innervate the prostatic stroma, capsule, bladder neck, and periurethral area, causing contraction and increased outlet resistance. The prostate is divided into zones. McNeal described the most commonly used division, which distinguishes the anterior, peripheral, transitional, and central zones.
Contraindications: Several general contraindications to all prostatic surgeries exist, such as active urinary infection or known or suspected prostate or urothelial cancer. Consider each of these before a treatment plan is instituted. Patients with neurogenic bladder voiding dysfunction should have their underlying neurogenic problem evaluated and treated.
Contraindications specific to TUMT are evolving as the technology changes and outcomes are studied further. Patients with a history of TURP or pelvic trauma should not undergo TUMT because of potential alterations in pelvic anatomy. Patients with glands that are smaller than 30 g or a prostatic urethral length of less than 3 cm respond poorly to TUMT, as do patients with glands greater than 100 g and patients with a prominent median bar.
Other contraindications include patients with metallic implants, penile prosthesis, severe urethral stricture disease, Leriche syndrome and/or severe peripheral vascular disease, or an artificial urinary sphincter. Patients with pacemakers need clearance from their cardiologists concerning turning their pacemakers off during therapy, although performing TUMT in this group should be approached with apprehension.
Hip replacement is no longer a contraindication. Acute urinary retention previously was thought to be a contraindication to TUMT. However, high-energy TUMT has shown promising results in this population, although efficacy has yet to be determined. Patients presenting in retention tend to be ill, with greater comorbidities; thus, they might benefit from the less invasive nature of TUMT."
Author Information Introduction Indications Relevant Anatomy And Contraindications Workup Treatment Complications Outcome And Prognosis Future And Controversies Pictures Bibliography
Relevant Anatomy: The urinary bladder is derived embryologically from the urogenital sinus. The detrusor musculature makes up the bulk of the bladder and is stimulated mainly by the parasympathetic nervous system. The ureters enter the bladder at the corners of the trigone. The prostate, which originates from the mesenchyme surrounding the urogenital sinus, is a compound tubuloalveolar gland whose base abuts the bladder neck and whose apex merges with the membranous urethra at the urogenital diaphragm. The normal adult gland is cone-shaped and is 4.4 cm in transverse diameter across the base, 3.4 cm in length, and 2.6 cm in anteroposterior direction. Its blood supply is from the prostatovesicular artery, a branch of the inferior vesical artery from the hypogastric artery.
The nerve supply is from the pelvic plexus, which travels with the prostatovesicular artery. Alpha-adrenergic nerves innervate the prostatic stroma, capsule, bladder neck, and periurethral area, causing contraction and increased outlet resistance. The prostate is divided into zones. McNeal described the most commonly used division, which distinguishes the anterior, peripheral, transitional, and central zones.
Contraindications: Several general contraindications to all prostatic surgeries exist, such as active urinary infection or known or suspected prostate or urothelial cancer. Consider each of these before a treatment plan is instituted. Patients with neurogenic bladder voiding dysfunction should have their underlying neurogenic problem evaluated and treated.
Contraindications specific to TUMT are evolving as the technology changes and outcomes are studied further. Patients with a history of TURP or pelvic trauma should not undergo TUMT because of potential alterations in pelvic anatomy. Patients with glands that are smaller than 30 g or a prostatic urethral length of less than 3 cm respond poorly to TUMT, as do patients with glands greater than 100 g and patients with a prominent median bar.
Other contraindications include patients with metallic implants, penile prosthesis, severe urethral stricture disease, Leriche syndrome and/or severe peripheral vascular disease, or an artificial urinary sphincter. Patients with pacemakers need clearance from their cardiologists concerning turning their pacemakers off during therapy, although performing TUMT in this group should be approached with apprehension.
Hip replacement is no longer a contraindication. Acute urinary retention previously was thought to be a contraindication to TUMT. However, high-energy TUMT has shown promising results in this population, although efficacy has yet to be determined. Patients presenting in retention tend to be ill, with greater comorbidities; thus, they might benefit from the less invasive nature of TUMT."
Johns Hopkins: Prostate including lifestyle measures to treat Benign Prostatic Hyperplasia (BPH)
Johns Hopkins: Prostate including lifestyle measures to treat Benign Prostatic Hyperplasia (BPH): "* During watchful waiting, you should adopt certain lifestyle measures to help relieve symptoms of mild Benign Prostatic Hyperplasia (BPH) and prevent them from worsening.
Doctors can’t predict how quickly an enlarged prostate will require treatment. Symptoms and objective measurements of obstruction in the urethra associated with benign prostatic hyperplasia (BPH) can remain stable for many years and may even improve over time in as many as a third of men. In one study from the Mayo Clinic, urinary symptoms did not worsen over a 3 1/2-year period in 73% of men with mild BPH.
Because the progression of and complications from BPH are unpredictable, watchful waiting—meaning that you are closely monitored but no immediate treatment is attempted—is best for men with minimal BPH symptoms that are not especially bothersome. With this treatment option for BPH, you only need to see your doctor about once a year to review the progress of symptoms and undergo a physical examination a few simple laboratory tests.
During watchful waiting, you should adopt certain lifestyle measures to help relieve symptoms of BPH and prevent them from worsening. For example, you should not take over-the-counter antihistamines and decongestants and should avoid delaying urination. If you have BPH you also need to be careful about your fluid intake by avoiding beverages that contain caffeine, limiting alcohol intake and the amount of fluid consumed at any one time, and avoiding beverages after 7 p.m.
Other helpful measures for these men with BPH include limiting spicy or salty foods, keeping warm, engaging in regular physical activity, and doing Kegel exercises (which involve squeezing and relaxing the pelvic floor muscles that support the bladder and surround the urethra)."
Doctors can’t predict how quickly an enlarged prostate will require treatment. Symptoms and objective measurements of obstruction in the urethra associated with benign prostatic hyperplasia (BPH) can remain stable for many years and may even improve over time in as many as a third of men. In one study from the Mayo Clinic, urinary symptoms did not worsen over a 3 1/2-year period in 73% of men with mild BPH.
Because the progression of and complications from BPH are unpredictable, watchful waiting—meaning that you are closely monitored but no immediate treatment is attempted—is best for men with minimal BPH symptoms that are not especially bothersome. With this treatment option for BPH, you only need to see your doctor about once a year to review the progress of symptoms and undergo a physical examination a few simple laboratory tests.
During watchful waiting, you should adopt certain lifestyle measures to help relieve symptoms of BPH and prevent them from worsening. For example, you should not take over-the-counter antihistamines and decongestants and should avoid delaying urination. If you have BPH you also need to be careful about your fluid intake by avoiding beverages that contain caffeine, limiting alcohol intake and the amount of fluid consumed at any one time, and avoiding beverages after 7 p.m.
Other helpful measures for these men with BPH include limiting spicy or salty foods, keeping warm, engaging in regular physical activity, and doing Kegel exercises (which involve squeezing and relaxing the pelvic floor muscles that support the bladder and surround the urethra)."
Johns Hopkins: Prostate Disorders on symptoms of BPH
Johns Hopkins: Prostate Disorders on symptoms of BPH: "Here’s an easy way to calculate whether you need treatment for benign prostatic hyperplasia (BPH).
The International Prostate Symptom Score questionnaire (see below) was developed by the American Urological Association to help men evaluate the severity of their symptoms from benign prostatic hyperplasia (BPH). This self-administered test can help determine which type of prostate treatment is needed, if any.
Instructions: Use this key to answer each question, then tabulate your score to assess your BPH severity.
Not at all = 0
Less than 1 time in 5 = 1
Less than half the time = 2
About half the time = 3
More than half the time = 4
Almost always = 5
* Over the past month, how often have you had the sensation of not emptying your bladder completely after you finished urinating?
* Over the past month, how often have you had to urinate again less than two hours after you finished urinating?
* Over the past month, how often have you found you stopped and started again several times when you urinated?
* Over the past month, how often have you found it difficult to postpone urination?
* Over the past month, how often have you had a weak urinary stream?
* Over the past month, how often have you had to push or strain to begin urination?
* Over the past month, how many times did you most typically get up to urinate from the time you went to bed at night until the time you got up in the morning?
Use your total score to assess BPH severity: mild BPH (1 to 7), moderate BPH (8 to 19), or severe BPH (20 to 35). Generally, no treatment is needed if symptoms are mild; moderate symptoms usually call for some form of BPH treatment; and severe symptoms indicate that surgery for BPH is most likely to be effective.
Posted in Prostate Disorders on October 11, 2006"
The International Prostate Symptom Score questionnaire (see below) was developed by the American Urological Association to help men evaluate the severity of their symptoms from benign prostatic hyperplasia (BPH). This self-administered test can help determine which type of prostate treatment is needed, if any.
Instructions: Use this key to answer each question, then tabulate your score to assess your BPH severity.
Not at all = 0
Less than 1 time in 5 = 1
Less than half the time = 2
About half the time = 3
More than half the time = 4
Almost always = 5
* Over the past month, how often have you had the sensation of not emptying your bladder completely after you finished urinating?
* Over the past month, how often have you had to urinate again less than two hours after you finished urinating?
* Over the past month, how often have you found you stopped and started again several times when you urinated?
* Over the past month, how often have you found it difficult to postpone urination?
* Over the past month, how often have you had a weak urinary stream?
* Over the past month, how often have you had to push or strain to begin urination?
* Over the past month, how many times did you most typically get up to urinate from the time you went to bed at night until the time you got up in the morning?
Use your total score to assess BPH severity: mild BPH (1 to 7), moderate BPH (8 to 19), or severe BPH (20 to 35). Generally, no treatment is needed if symptoms are mild; moderate symptoms usually call for some form of BPH treatment; and severe symptoms indicate that surgery for BPH is most likely to be effective.
Posted in Prostate Disorders on October 11, 2006"
Johns Hopkins: Prostate on BPH treatment options, Possible Complications
Johns Hopkins: Prostate on BPH treatment options: "Possible Complications
While minimally invasive procedures for BPH are often associated with less severe complications than TURP, they still can cause side effects, including the following:
* Difficult or painful urination. These problems are common in the first days after the catheter is removed, but they typically improve after a week or two. If urinating is extremely painful or does not improve, contact your urologist.
* Blood in the urine. A small amount of blood that lends a pinkish hue to your urine may cause you some anxiety but is common for up to three days after the procedure. However, if the bleeding is heavy, lasts more than a few days, or causes blood clots that block the flow of urine, call your urologist.
* Urinary tract infections. These infections usually result from catheterization; the longer you have a catheter, the higher your risk of infection. To reduce this risk, antibiotics are often prescribed either after the procedure or after catheter removal.
* Urinary retention. A small number of BPH patients are unable to urinate on their own after catheter removal and may require a longer period of catheterization. If this happens, contact your doctor.
* Sexual dysfunction. In general, the rates of sexual dysfunction are thought to be lower with TUNA and TUMT than with TURP. Nonetheless, men can experience retrograde ejaculation (ejaculation into the bladder instead of through the penis) after TUNA and TUMT. In one study, one in five men reported retrograde ejaculation after TUMT. However, most studies show that TUNA and TUMT have no major adverse effects on sexual function.
* Severe abdominal pain or a high fever. Contact your doctor if you experience either of these symptoms."
While minimally invasive procedures for BPH are often associated with less severe complications than TURP, they still can cause side effects, including the following:
* Difficult or painful urination. These problems are common in the first days after the catheter is removed, but they typically improve after a week or two. If urinating is extremely painful or does not improve, contact your urologist.
* Blood in the urine. A small amount of blood that lends a pinkish hue to your urine may cause you some anxiety but is common for up to three days after the procedure. However, if the bleeding is heavy, lasts more than a few days, or causes blood clots that block the flow of urine, call your urologist.
* Urinary tract infections. These infections usually result from catheterization; the longer you have a catheter, the higher your risk of infection. To reduce this risk, antibiotics are often prescribed either after the procedure or after catheter removal.
* Urinary retention. A small number of BPH patients are unable to urinate on their own after catheter removal and may require a longer period of catheterization. If this happens, contact your doctor.
* Sexual dysfunction. In general, the rates of sexual dysfunction are thought to be lower with TUNA and TUMT than with TURP. Nonetheless, men can experience retrograde ejaculation (ejaculation into the bladder instead of through the penis) after TUNA and TUMT. In one study, one in five men reported retrograde ejaculation after TUMT. However, most studies show that TUNA and TUMT have no major adverse effects on sexual function.
* Severe abdominal pain or a high fever. Contact your doctor if you experience either of these symptoms."
Microwave Thermotherapy (TUMT) Systems - Urology Product Comparison - Medcompare
Microwave Thermotherapy (TUMT) Systems - Urology Product Comparison - Medcompare: "Item
CoreTherm™ Microwave Thermotherapy System
The Targis® System
The Prostatron® System
TherMatrx® Dose Optimized Thermotherapy™
Prolieve™ Thermodilatation System
The CoreTherm Microwave Thermotherapy System is the Next Generation thermotherapy device for the treatment of symptomatic BPH. Other thermotherapy systems treat patients on standard treatment protocols, discounting the effect of each patient's individual intraprostatic ...
More...
The Targis® System uses Cooled ThermoTherapy® (transurethral microwave thermotherapy -TUMT®) to deliver precisely targeted microwave energy deep into hyperplastic prostate tissue creating coagulative necrosis for durable clinical outcomes. Dual parameter ...
More...
The Prostatron® System uses Cooled ThermoTherapy® (transurethral microwave thermotherapy -TUMT®) to deliver precisely targeted microwave energy to heat and destroy hyperplastic prostate tissue while a unique cooling mechanism simultaneously protects surrounding ...
More...
TherMatrx® Dose Optimized Thermotherapy™ is an advanced transurethral microwave thermotherapy system designed for in-office treatment of benign prostate hyperplasia (BPH). TherMatrx is the most widely used in-office BPH thermotherapy treatment in the United ...
More...
The Prolieve System is the next generation in minimally invasive therapy for the symptoms of BPH. This dual-action thermodilatation technology simultaneously heats the prostate while dilating the prostatic urethra. The treatment is well tolerated by patients and most ...
More..."
CoreTherm™ Microwave Thermotherapy System
The Targis® System
The Prostatron® System
TherMatrx® Dose Optimized Thermotherapy™
Prolieve™ Thermodilatation System
The CoreTherm Microwave Thermotherapy System is the Next Generation thermotherapy device for the treatment of symptomatic BPH. Other thermotherapy systems treat patients on standard treatment protocols, discounting the effect of each patient's individual intraprostatic ...
More...
The Targis® System uses Cooled ThermoTherapy® (transurethral microwave thermotherapy -TUMT®) to deliver precisely targeted microwave energy deep into hyperplastic prostate tissue creating coagulative necrosis for durable clinical outcomes. Dual parameter ...
More...
The Prostatron® System uses Cooled ThermoTherapy® (transurethral microwave thermotherapy -TUMT®) to deliver precisely targeted microwave energy to heat and destroy hyperplastic prostate tissue while a unique cooling mechanism simultaneously protects surrounding ...
More...
TherMatrx® Dose Optimized Thermotherapy™ is an advanced transurethral microwave thermotherapy system designed for in-office treatment of benign prostate hyperplasia (BPH). TherMatrx is the most widely used in-office BPH thermotherapy treatment in the United ...
More...
The Prolieve System is the next generation in minimally invasive therapy for the symptoms of BPH. This dual-action thermodilatation technology simultaneously heats the prostate while dilating the prostatic urethra. The treatment is well tolerated by patients and most ...
More..."
Transurethral Microwave Technology (TUMT)
Transurethral Microwave Technology (TUMT): "Transurethral Microwave Technology (TUMT)
Transurethral Microwave Technology (TUMT)
Transurethral Microwave Technology (TUMT) shrinks prostate tissue using heat from a microwave device. Usually several sessions are needed to shrink the tissue.
You will be given a sedative before the procedure. A catheter (a tube running from your bladder outside your body) will be put in place before the procedure. A device that sends computer-regulated microwaves through the catheter is used to heat selected portions of the prostate to at least 111° Fahrenheit. A cooling system protects the urinary tract during the procedure.
The tissues are heated for 30 to 60 minutes each session. This is an outpatient procedure. The catheter will be left in place five to seven days.
TUMT has not been reported to lead to impotence or incontinence.
Microwave therapy doesn't cure an enlarged prostate (benign prostatic hyperplasia), but it does reduce most symptoms. It doesn't, however correct the problem of incomplete emptying of the bladder.
Re-evaluations are needed from time to time to check the status of your prostate (and rule out prostate cancer). This follow-up - while available at the Minimally Invasive Urology Institute - is usually done by your own urologist."
Transurethral Microwave Technology (TUMT)
Transurethral Microwave Technology (TUMT) shrinks prostate tissue using heat from a microwave device. Usually several sessions are needed to shrink the tissue.
You will be given a sedative before the procedure. A catheter (a tube running from your bladder outside your body) will be put in place before the procedure. A device that sends computer-regulated microwaves through the catheter is used to heat selected portions of the prostate to at least 111° Fahrenheit. A cooling system protects the urinary tract during the procedure.
The tissues are heated for 30 to 60 minutes each session. This is an outpatient procedure. The catheter will be left in place five to seven days.
TUMT has not been reported to lead to impotence or incontinence.
Microwave therapy doesn't cure an enlarged prostate (benign prostatic hyperplasia), but it does reduce most symptoms. It doesn't, however correct the problem of incomplete emptying of the bladder.
Re-evaluations are needed from time to time to check the status of your prostate (and rule out prostate cancer). This follow-up - while available at the Minimally Invasive Urology Institute - is usually done by your own urologist."
Medicare Part B - KS/NE/W.MO - TUMT
Medicare Part B - KS/NE/W.MO - TUMT: "Revision Effective Date
08/16/2006 Revision Ending Date
Indications and Limitations of Coverage and/or Medical Necessity
Transurethral Microwave Thermotherapy (TUMT) is a non-surgical approach for the treatment of symptomatic benign prostatic hyperplasia. Thermotherapy uses temperatures above 45 0 C to destroy excess prostatic tissue causing outlet obstruction.
Thermotherapy is currently covered by Medicare only for treatment of outlet obstruction caused by benign prostatic hyperplasia.
Reasons for Non-Coverage
The safety and efficacy of Microwave Thermotherapy of other prostatic conditions has not been established at this time and are, therefore, not covered by Medicare."
08/16/2006 Revision Ending Date
Indications and Limitations of Coverage and/or Medical Necessity
Transurethral Microwave Thermotherapy (TUMT) is a non-surgical approach for the treatment of symptomatic benign prostatic hyperplasia. Thermotherapy uses temperatures above 45 0 C to destroy excess prostatic tissue causing outlet obstruction.
Thermotherapy is currently covered by Medicare only for treatment of outlet obstruction caused by benign prostatic hyperplasia.
Reasons for Non-Coverage
The safety and efficacy of Microwave Thermotherapy of other prostatic conditions has not been established at this time and are, therefore, not covered by Medicare."
Transurethral microwave therapy (TUMT) for benign prostatic hyperplasia
Transurethral microwave therapy (TUMT) for benign prostatic hyperplasia:
"TUMT is done to help relieve the symptoms of benign prostatic hyperplasia (BPH). It is an option for men who want more than medications for treatment of their symptoms.
How Well It Works
Studies note that TUMT is more effective than treatment with the alpha-blocker terazosin when checked 18 months later.1
TUMT improved symptoms more than transurethral resection of the prostate (TURP) in one study but not in two others.
1
Risks
The main complication of TUMT is the inability to urinate (urinary retention) for more than a week.2 This condition is treated by inserting a tube directly through the abdominal wall into the bladder to drain urine (suprapubic catheter). Erection problems and retrograde ejaculation (ejaculation backward into the bladder) appear less common after TUMT than after TURP.2
Other complications include persistent irritation of the urethra and blood in the urine.1
Recent reports have warned that the procedure has in a small number of cases caused serious injuries and complications, including damage to the penis and urethra. Injuries have required colostomies, partial amputation of the penis, and other procedures. In December 2000, the U.S. Food and Drug Administration (FDA) issued a warning on these injuries.3
What To Think About
Most trials using TUMT have been limited by a small number of participants, a short length of time of study, and limited follow-up of the participants after the trial ended.1"
"TUMT is done to help relieve the symptoms of benign prostatic hyperplasia (BPH). It is an option for men who want more than medications for treatment of their symptoms.
How Well It Works
Studies note that TUMT is more effective than treatment with the alpha-blocker terazosin when checked 18 months later.1
TUMT improved symptoms more than transurethral resection of the prostate (TURP) in one study but not in two others.
1
Risks
The main complication of TUMT is the inability to urinate (urinary retention) for more than a week.2 This condition is treated by inserting a tube directly through the abdominal wall into the bladder to drain urine (suprapubic catheter). Erection problems and retrograde ejaculation (ejaculation backward into the bladder) appear less common after TUMT than after TURP.2
Other complications include persistent irritation of the urethra and blood in the urine.1
Recent reports have warned that the procedure has in a small number of cases caused serious injuries and complications, including damage to the penis and urethra. Injuries have required colostomies, partial amputation of the penis, and other procedures. In December 2000, the U.S. Food and Drug Administration (FDA) issued a warning on these injuries.3
What To Think About
Most trials using TUMT have been limited by a small number of participants, a short length of time of study, and limited follow-up of the participants after the trial ended.1"
TUMT (transurethral microwave thermotherapy) available in Orange County
TUMT (transurethral microwave thermotherapy) now available in Orange County: "TUMT is a covered procedure by many leading health insurers. It is best to check each patient's insurance policy to make sure that TUMT is a covered procedure as Individual policies can vary from patient to patient.
The following insurance carriers cover TUMT. (There could be an exclusion to an individual patient's policy, although this is rare)
Medicare
Aetna
CIGNA
Blue Cross
Blue Shield
Beech Street
PHCS
United Healthcare
Pacificare
For more information regarding TUMT, please contact Associated Urologists of Orange County."
The following insurance carriers cover TUMT. (There could be an exclusion to an individual patient's policy, although this is rare)
Medicare
Aetna
CIGNA
Blue Cross
Blue Shield
Beech Street
PHCS
United Healthcare
Pacificare
For more information regarding TUMT, please contact Associated Urologists of Orange County."
Opinions on TUMT procedure? [BPH]
Opinions on TUMT procedure? [BPH]: "About age - if you had a 5 year old house and the plumbing backed up,
would you think 'this house is too new for roto-rooter so I'll live with
it and mop up everyday until it's 20 years older?'
Look up posts to this NG from Patrick starting 4 or 5 years ago. He was
around your age, had serious BPH and had an unsuccessful microwave
treatment for it. Several of his Doctors and Urologists did not want to
believe it could be BPH at his age. He finally became an early
participant in clinical trials of PVP. His results were great and
influenced a few of us on this NG to seek PVP.
Left untreated, BPH can do permanent damage to your bladder and even
kidneys - just like ignoring a plumbing leak can eventually cause rot,
mildew and mold.
I believe that the reason some guys have continuing problems after PVP,
and some other procedures, is because things above the prostate have
become damaged by neglect. Clearing the passageway cannot restore a
bladder stretched and weakened by years of retention. Good Doctors
explain what you can reasonably expect, based on the tests and
evaluation they have performed on you, before scheduling surgery.
My advice is to thoroughly evaluate through urodynamic tests,
cystoscophy, blood work, PSA (with biopsy if indicated) what and where
the problem really is. If you indeed have BPH - fix it. I am among
those extremely satisfied and grateful for my PVP - but I would add that
I would rather have a TURP by the best TURP surgeon in the country than
a PVP by the worst PVP surgeon. The skill of my surgeon fixed my BPH.
Al
PVP Dec 2003, Dr Te
N D via MedKB.com wrote:
> Hi, I'm a 34-year-old who has been dealing with moderate BPH the past few
> years. Tried Flomax and Urotraxal and had bad reactions to them, and after
> conssulting with 2 uros have opted to get trans urethral microwave therapy
> done in January rather than anything more invasive which I'd like to avoid
> since I'm pretty young for all this. Long story short, would like to get
> opinions from anyone that may have had it done. Hard to find real experiences
> and opinions out there on the Internet on this. I'd like to hear anyone's
> experiences if they have them. Thanks!"
would you think 'this house is too new for roto-rooter so I'll live with
it and mop up everyday until it's 20 years older?'
Look up posts to this NG from Patrick starting 4 or 5 years ago. He was
around your age, had serious BPH and had an unsuccessful microwave
treatment for it. Several of his Doctors and Urologists did not want to
believe it could be BPH at his age. He finally became an early
participant in clinical trials of PVP. His results were great and
influenced a few of us on this NG to seek PVP.
Left untreated, BPH can do permanent damage to your bladder and even
kidneys - just like ignoring a plumbing leak can eventually cause rot,
mildew and mold.
I believe that the reason some guys have continuing problems after PVP,
and some other procedures, is because things above the prostate have
become damaged by neglect. Clearing the passageway cannot restore a
bladder stretched and weakened by years of retention. Good Doctors
explain what you can reasonably expect, based on the tests and
evaluation they have performed on you, before scheduling surgery.
My advice is to thoroughly evaluate through urodynamic tests,
cystoscophy, blood work, PSA (with biopsy if indicated) what and where
the problem really is. If you indeed have BPH - fix it. I am among
those extremely satisfied and grateful for my PVP - but I would add that
I would rather have a TURP by the best TURP surgeon in the country than
a PVP by the worst PVP surgeon. The skill of my surgeon fixed my BPH.
Al
PVP Dec 2003, Dr Te
N D via MedKB.com wrote:
> Hi, I'm a 34-year-old who has been dealing with moderate BPH the past few
> years. Tried Flomax and Urotraxal and had bad reactions to them, and after
> conssulting with 2 uros have opted to get trans urethral microwave therapy
> done in January rather than anything more invasive which I'd like to avoid
> since I'm pretty young for all this. Long story short, would like to get
> opinions from anyone that may have had it done. Hard to find real experiences
> and opinions out there on the Internet on this. I'd like to hear anyone's
> experiences if they have them. Thanks!"
Transurethral Microwave Technology (TUMT)
Transurethral Microwave Technology (TUMT): "TUMT has not been reported to lead to impotence or incontinence.
Microwave therapy doesn't cure an enlarged prostate (benign prostatic hyperplasia), but it does reduce most symptoms. It doesn't, however correct the problem of incomplete emptying of the bladder.
Re-evaluations are needed from time to time to check the status of your prostate (and rule out prostate cancer). This follow-up - while available at the Minimally Invasive Urology Institute - is usually done by your own urologist."
Microwave therapy doesn't cure an enlarged prostate (benign prostatic hyperplasia), but it does reduce most symptoms. It doesn't, however correct the problem of incomplete emptying of the bladder.
Re-evaluations are needed from time to time to check the status of your prostate (and rule out prostate cancer). This follow-up - while available at the Minimally Invasive Urology Institute - is usually done by your own urologist."
Urology of Indiana > Current Patients > Instructions > Post TUMT Discharge Instructions
Urology of Indiana > Current Patients > Instructions > Post TUMT Discharge Instructions: "Post TUMT Discharge Instructions
General Expectations
Some men may experience discomfort after treatment. On occasion, some bloody discharge may be apparent from the penis. You may have soreness in the lower abdomen, and it may be uncomfortable to sit. You may experience urgency and frequency when urinating. These are all normal reactions to the treatment.
Post TUMT Instructions:
1. Have someone drive you home after the procedure and do not drive until the catheter is removed.
2. Drink plenty of water.
3. Do not engage in strenuous activity for at least a week.
4. Abstain from sexual activity for two weeks.
5. You may take a shower. Avoid a bath until your catheter has been removed.
6. Take your medications as prescribed.
7. Because of some of the medications administered during procedure, do not consume alcohol, sedatives or stimulants for 24 hours. Also report any dizziness, slurred speech or altered sensation. An adult should remain with you for the rest of the day.
Complications
You should contact your physician if you experience any of the following:
1. Temperature of 101 degrees taken by mouth
2. Excessive urinary bleeding or bleeding from the penis
3. Bladder spasms that are continuous
4. No urine drains into the bag for more than 4 hours
5. Nausea and vomiting
If problems occur please call the on call physician at the number provided below. If for some reason you are unable to reach the physician you may go to the hospital emergency room. If you do go to the emergency room for catheterization, be sure to tell them to use a Coude (pronounced coo-day) tipped catheter.
Post treatment medication management:
1. Continue current prostate medications: Flomax, Cardura(Doxazosin),or Hytrin(Terazosin)
2. Take antibiotic as prescribed
3. Take anti-inflammatory medication if prescribed.
4. Pain medication as prescribed.
* Please review attached catheter care instruction sheet."
General Expectations
Some men may experience discomfort after treatment. On occasion, some bloody discharge may be apparent from the penis. You may have soreness in the lower abdomen, and it may be uncomfortable to sit. You may experience urgency and frequency when urinating. These are all normal reactions to the treatment.
Post TUMT Instructions:
1. Have someone drive you home after the procedure and do not drive until the catheter is removed.
2. Drink plenty of water.
3. Do not engage in strenuous activity for at least a week.
4. Abstain from sexual activity for two weeks.
5. You may take a shower. Avoid a bath until your catheter has been removed.
6. Take your medications as prescribed.
7. Because of some of the medications administered during procedure, do not consume alcohol, sedatives or stimulants for 24 hours. Also report any dizziness, slurred speech or altered sensation. An adult should remain with you for the rest of the day.
Complications
You should contact your physician if you experience any of the following:
1. Temperature of 101 degrees taken by mouth
2. Excessive urinary bleeding or bleeding from the penis
3. Bladder spasms that are continuous
4. No urine drains into the bag for more than 4 hours
5. Nausea and vomiting
If problems occur please call the on call physician at the number provided below. If for some reason you are unable to reach the physician you may go to the hospital emergency room. If you do go to the emergency room for catheterization, be sure to tell them to use a Coude (pronounced coo-day) tipped catheter.
Post treatment medication management:
1. Continue current prostate medications: Flomax, Cardura(Doxazosin),or Hytrin(Terazosin)
2. Take antibiotic as prescribed
3. Take anti-inflammatory medication if prescribed.
4. Pain medication as prescribed.
* Please review attached catheter care instruction sheet."
Mailgate: sci.med.prostate.bph: Re: TUMT post effects
Mailgate: sci.med.prostate.bph: Re: TUMT post effects: "Joe, I had TUMT on Dec 3 last year. Mine was the Targis which took 30 minutes. It was (for me) extremely painful. I was given a valium and vicodin prior to the procedure but they didn't seem to make much difference. I also experienced a great deal of post-op pain for two months!! I was told that I was the only patient that experienced that much discomfort. So perhaps I was an exception to the norm. I took out the catheter the day after the procedure because I hated the damned thing. I could barely pee for the next couple days so I probably shouldn't have done that. I experienced bleeding during voiding for a good six weeks. When I ejaculated what came out looked like tabasco sauce! So don't be alarmed should you do that. It goes back to normal in time. The good news is that by week five I was peeing quite well. It is now 3 1/2 months and I am peeing very well. The pain is now gone. Even if I am sitting in a long meeting and have to pee BAD, when I do get to the bathroom it just flows! Used to be if I held it too long I could take over five minutes to void. And even then it was not complete and I would have to return to the bathroom in 10 minutes. I hated that! So, inspite of the discomfort I experienced, I am very happy now. I just hope that the effects last for many years. Good Luck! Bob"
BPH Doctor - Boise, Weiser, Idaho, Ontario, Baker City, Oregon - Urologist Marc Iseri, MD - TUMT, Cooled Thermotherapy
BPH Doctor - Boise, Weiser, Idaho, Ontario, Baker City, Oregon - Urologist Marc Iseri, MD - TUMT, Cooled Thermotherapy: "Iseri and Associates Urology - Dr. Marc Iseri, Urologist, vasectomy services in Boise, Idaho, Weiser, Idaho, Ontario, Oregon, and Baker City, Oregon
Cooled ThermoTherapy™ (TUMT)
There are a number of treatments available for enlarged prostate. Understanding the advantages and disadvantages of each treatment will help you decide which treatment is right for you. Discuss this information with your urologist.
Non-Surgical Treatments
There are a number of non-surgical treatment options for BPH. One type of non-surgical treatment is thermotherapy, which uses various energy sources to heat and destroy enlarged prostate tissue.
Cooled ThermoTherapy™ is a single, non-surgical, office-based treatment for BPH that uses microwave energy to heat and destroy enlarged prostate tissue. Unlike other treatments, Cooled ThermoTherapy™ uses cooling technology to minimize discomfort to the patient during the treatment. Cooled ThermoTherapy™ has been FDA approved since 1996.
Medication
medication
Medication is often the first-line treatment against enlarged prostate symptoms. However, drugs must be taken once or twice a day for the rest of your life. Over time, the cost can become a large expense and drugs are not effective for all patients. Side effects may include fatigue, headache, dizziness, impotence and loss of sex drive.
Significant cost of lifetime use of current medications – if you stop taking them they stop working. Over 50% of patients who start a regimen of medications for BPH discontinue the treatment within three years ¹.
Surgery
surgery
Surgery may be considered when symptoms have not improved with other treatments. It removes large amounts of prostate tissue and is performed in a hospital or surgical center and requires anesthesia. Surgery carries the risk of complications, including retrograde ejaculation, impotence and incontinence."
Cooled ThermoTherapy™ (TUMT)
There are a number of treatments available for enlarged prostate. Understanding the advantages and disadvantages of each treatment will help you decide which treatment is right for you. Discuss this information with your urologist.
Non-Surgical Treatments
There are a number of non-surgical treatment options for BPH. One type of non-surgical treatment is thermotherapy, which uses various energy sources to heat and destroy enlarged prostate tissue.
Cooled ThermoTherapy™ is a single, non-surgical, office-based treatment for BPH that uses microwave energy to heat and destroy enlarged prostate tissue. Unlike other treatments, Cooled ThermoTherapy™ uses cooling technology to minimize discomfort to the patient during the treatment. Cooled ThermoTherapy™ has been FDA approved since 1996.
Medication
medication
Medication is often the first-line treatment against enlarged prostate symptoms. However, drugs must be taken once or twice a day for the rest of your life. Over time, the cost can become a large expense and drugs are not effective for all patients. Side effects may include fatigue, headache, dizziness, impotence and loss of sex drive.
Significant cost of lifetime use of current medications – if you stop taking them they stop working. Over 50% of patients who start a regimen of medications for BPH discontinue the treatment within three years ¹.
Surgery
surgery
Surgery may be considered when symptoms have not improved with other treatments. It removes large amounts of prostate tissue and is performed in a hospital or surgical center and requires anesthesia. Surgery carries the risk of complications, including retrograde ejaculation, impotence and incontinence."
Enlarged Prostate and TUMT
Enlarged Prostate and TUMT: "Dear DoctorInternet - Enlarged Prostate and TUMT
(February 3, 2001)
B.G. 'Although I underwent a TUMT six months ago I have not appreciably improved despite early signs of stronger urine flow. Whether this is due to age (69 years) or reduced bladder capacity or prostate restrictions I don't yet know. The answer would be very helpful.'
DoctorInternet. First some background. TUMT stands for 'TransUrethral Microwave Thermotherapy to prostate'. This is a minimally invasive treatment which aims at alleviating the difficulty in urination which is associated with non-malignant, enlarged prostate or Benign Prostatic Hypertrophy (BHP). The treatment causes a destruction of prostatic tissue by microwave heating and thus relieves the constriction around the urethra which causes the difficulty with urination. Although most, minimally invasive treatments for this condition seem to be abandoned after controlled studies, TUMT has survived as a common practice in urology. The more direct procedure and 'gold standard' is 'Transurethral Resection of the Prostate' (TURP) - a surgical technique, which requires greater technical skill, is more expensive, and can have more adverse effects. Other treatment options include: watchful waiting, balloon dilation, prostatic stent, medication (such as finasteride and terazosin), and the herb, serenoa repens. BPH is, essentially, inevitable with biological ageing. Over 50% of males over age 50 report varying degrees of the symptoms and by the age of 80, almost 90% have the underlying pathology.
Now, with respect to the particular question about why TUMT had only a transient benefit to the correspondent, studies have shown that, within the first year after treatment by TUMT, some 38% of the patients are dissatisfied with the results and that within 4 years after the procedure, the percentage who are dissatisfied increases to 77%. Thus, there is a high rate of only short term benefits. Other studies seem to show better and longer lasting results. As in most therapies, efficacy depends on the appropriateness of the treatment for the pathology of the particular person and the skill of the therapist. The procedure can be redone or alternatives attempted.
In addressing this inquiry, DoctorInternet exchanged e-mails with B.G., one of which was amusing. DoctorInternet to B.G. 'Incidentally, I forgot to ask your height and weight'. B.G. replied: 'My height is 5'10' and I weigh 210; and yes I already know, I'm too short'. (Bringing one's weight to its optimum improves virtually all disorders.)"
(February 3, 2001)
B.G. 'Although I underwent a TUMT six months ago I have not appreciably improved despite early signs of stronger urine flow. Whether this is due to age (69 years) or reduced bladder capacity or prostate restrictions I don't yet know. The answer would be very helpful.'
DoctorInternet. First some background. TUMT stands for 'TransUrethral Microwave Thermotherapy to prostate'. This is a minimally invasive treatment which aims at alleviating the difficulty in urination which is associated with non-malignant, enlarged prostate or Benign Prostatic Hypertrophy (BHP). The treatment causes a destruction of prostatic tissue by microwave heating and thus relieves the constriction around the urethra which causes the difficulty with urination. Although most, minimally invasive treatments for this condition seem to be abandoned after controlled studies, TUMT has survived as a common practice in urology. The more direct procedure and 'gold standard' is 'Transurethral Resection of the Prostate' (TURP) - a surgical technique, which requires greater technical skill, is more expensive, and can have more adverse effects. Other treatment options include: watchful waiting, balloon dilation, prostatic stent, medication (such as finasteride and terazosin), and the herb, serenoa repens. BPH is, essentially, inevitable with biological ageing. Over 50% of males over age 50 report varying degrees of the symptoms and by the age of 80, almost 90% have the underlying pathology.
Now, with respect to the particular question about why TUMT had only a transient benefit to the correspondent, studies have shown that, within the first year after treatment by TUMT, some 38% of the patients are dissatisfied with the results and that within 4 years after the procedure, the percentage who are dissatisfied increases to 77%. Thus, there is a high rate of only short term benefits. Other studies seem to show better and longer lasting results. As in most therapies, efficacy depends on the appropriateness of the treatment for the pathology of the particular person and the skill of the therapist. The procedure can be redone or alternatives attempted.
In addressing this inquiry, DoctorInternet exchanged e-mails with B.G., one of which was amusing. DoctorInternet to B.G. 'Incidentally, I forgot to ask your height and weight'. B.G. replied: 'My height is 5'10' and I weigh 210; and yes I already know, I'm too short'. (Bringing one's weight to its optimum improves virtually all disorders.)"
eMedicine - Transurethral Microwave Thermotherapy of the Prostate (TUMT) : Article by Jonathan Rubenstein, MD
eMedicine - Transurethral Microwave Thermotherapy of the Prostate (TUMT) : Article by Jonathan Rubenstein, MD: "One (of many) minimally invasive methods for the treatment of symptomatic BPH is transurethral microwave thermotherapy (TUMT). TUMT involves the insertion of a specially designed Foley-type catheter into the bladder, allowing a microwave antenna to be positioned within the prostatic fossa. Microwaves are then created to heat and destroy the hyperplastic prostate tissue. The goal of microwave therapy is to provide a one-time efficacious treatment of LUTS due to BPH, avoiding the risk associated with TURP or open prostatic enucleation and avoiding the need to take medicines daily and the risk associated with pharmacotherapy. Early results show excellent symptomatic relief, although long-term follow-up data are not yet available and the improvement is often less than that after TURP. The technology and results after TUMT continue to evolve."
Subscribe to:
Posts (Atom)